

Guideline-Concordant Antiviral Treatment in Children at High Risk for Influenza Complications
- PMID: 35867691
- PMCID: PMC10169402
- DOI: 10.1093/cid/ciac606
Guideline-Concordant Antiviral Treatment in Children at High Risk for Influenza Complications
Abstract
Background: National guidelines recommend antiviral treatment for children with influenza at high risk for complications regardless of symptom duration. Little is known about concordance of clinical practice with this recommendation.
Methods: We performed a cross-sectional study of outpatient children (aged 1-18 years) at high risk for complications who were diagnosed with influenza during the 2016-2019 influenza seasons. High-risk status was determined using an existing definition that includes age, comorbidities, and residence in a long-term care facility. The primary outcome was influenza antiviral dispensing within 2 days of influenza diagnosis. We determined patient- and provider-level factors associated with guideline-concordant treatment using multivariable logistic regression.
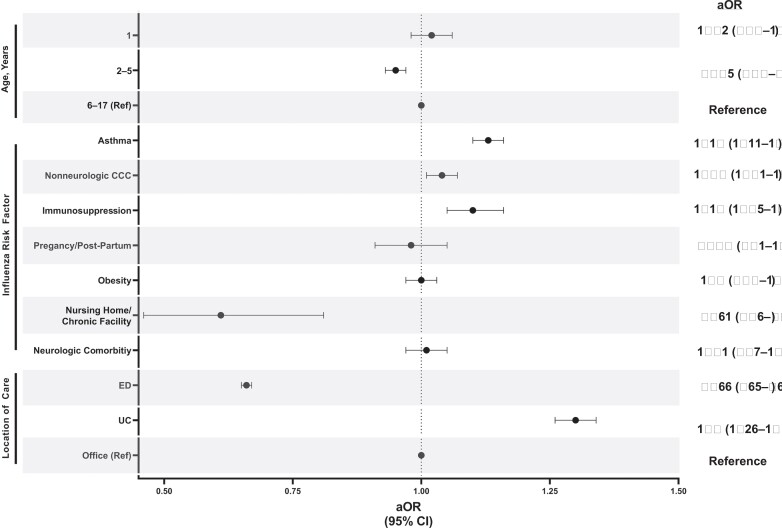
Results: Of the 274 213 children with influenza at high risk for influenza complications, 159 350 (58.1%) received antiviral treatment. Antiviral treatment was associated with the presence of asthma (aOR, 1.13; 95% confidence interval [CI], 1.11-1.16), immunosuppression (aOR, 1.10; 95% CI, 1.05-1.16), complex chronic conditions (aOR, 1.04; 95% CI, 1.01-1.07), and index encounter in the urgent care setting (aOR, 1.3; 95% CI, 1.26-1.34). Factors associated with decreased odds of antiviral treatment include age 2-5 years compared with 6-17 years (aOR, 0.95; 95% CI, .93-.97), residing in a chronic care facility (aOR, .61; 95% CI, .46-.81), and index encounter in an emergency department (aOR, 0.66; 95% CI, .63-.71).
Conclusions: Among children with influenza at high risk for complications, 42% did not receive guideline-concordant antiviral treatment. Further study is needed to elucidate barriers to appropriate use of antivirals in this vulnerable population.
Keywords: antiviral; influenza; oseltamivir; pediatrics.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest . C. G. G. has received consulting fees from Pfizer, Sanofi, and Merck and grants or contracts paid to their institution from Campbell Alliance/Syneos Health, Sanofi, the Centers for Disease Control and Prevention (CDC), Agency for Healthcare Research and Quality (AHRQ), NIH, and US Food and Drug Administration. D. J. W. has received in-kind research support from bioMérieux and reports grants or contracts paid to their institution from NIAID, CDC, Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), and National Heart, Lung, and Blood Institute (NHLBI); served as division chief of the Division of Hospital Medicine, Vanderbilt University Medical Center; and served on the Executive Committee–Pediatric Research in Inpatient Setting. J. W. A. reports grants or contracts unrelated to this work from a Turner Hazinski Research Award–Vanderbilt University Medical Center, Young Investigator Award–Academic Pediatric Association, Maternal and Pediatric Precision in Therapeutics (MPRINT) Hub Pilot Funding–NIH NICHD, and an NIH NHLBI K12 award, all paid to their institution; and payment to author for expert testimony from Lewis Rice, LLC, unrelated to this work. J. L. G. reports grants or contracts from the NICDH and the National Institute of General Medical Sciences unrelated to this work and paid to their institution and payment or honoraria paid to author from the American Academy of Pediatrics (presentation) and the Missouri Association of School Nurses (honoraria). S. T. G. reports a Gerber Foundation Novice Research Award and Eunice Kennedy Shriver National Institute of Child Health and Human Development award unrelated to this work; participation on a University of Cincinnati data and safety monitoring board for an NICHD R01-funded protocol; and serving as a member of the American Society of Clinical Pharmacology & Therapeutics (ASCPT) By Laws Committee, ASCPT Scientific Programming Committee, and ASCPT Career Development. S. S. S. reports grant funding from the Children’s Hospital Association to their institution to develop a quality dashboard and grant funding to institution from Patient-Centered Outcomes Research Institute and AHRQ. All remaining authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Blyth CC, Macartney KK, McRae J, et al. . Influenza epidemiology, vaccine coverage and vaccine effectiveness in children admitted to sentinel Australian hospitals in 2017: results from the PAEDS-FluCAN Collaboration. Clin Infect Dis 2019; 68:940–8. - PubMed
-
- Burton C, Vaudry W, Moore D, et al. . Burden of seasonal influenza in children with neurodevelopmental conditions. Pediatr Infect Dis J 2014; 33:710–4. - PubMed
-
- Chaves SS, Perez A, Farley MM, et al. . The burden of influenza hospitalizations in infants from 2003 to 2012, United States. Pediatr Infect Dis J 2014; 33:912–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
