

SARS-CoV-2 triggers pericyte-mediated cerebral capillary constriction
- PMID: 35867861
- PMCID: PMC9384509
- DOI: 10.1093/brain/awac272
SARS-CoV-2 triggers pericyte-mediated cerebral capillary constriction
Abstract
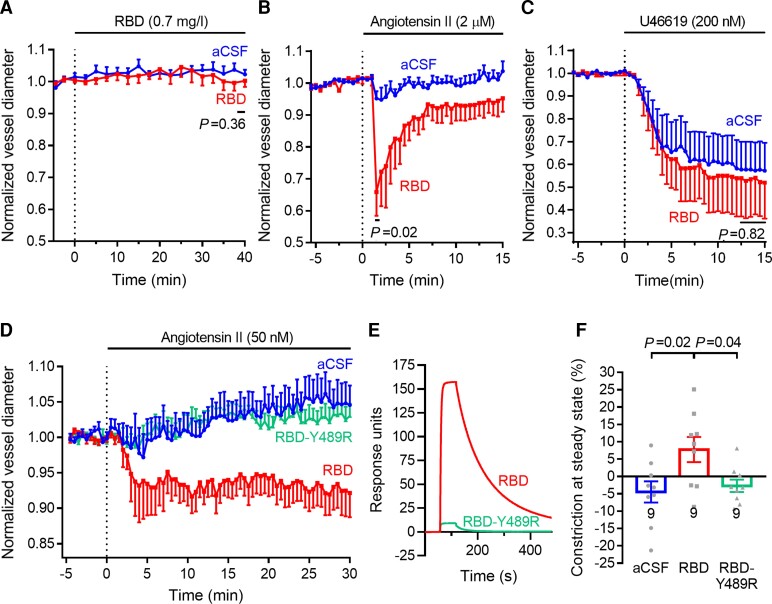
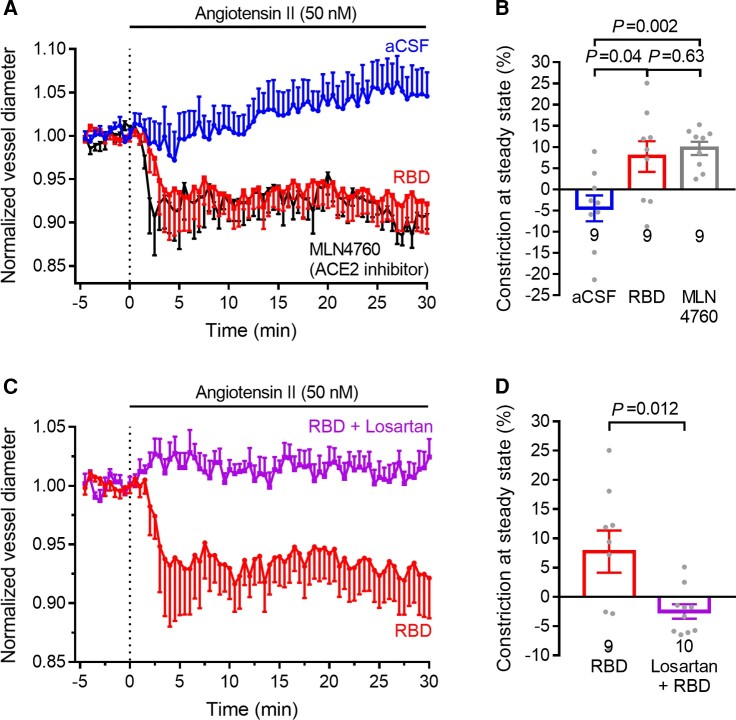
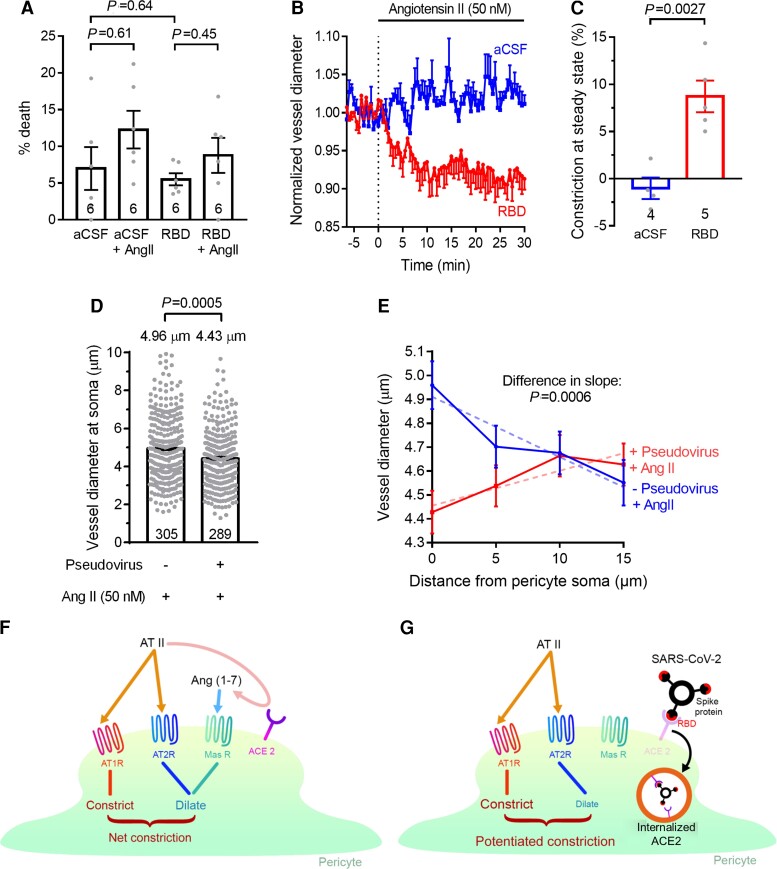
The SARS-CoV-2 receptor, ACE2, is found on pericytes, contractile cells enwrapping capillaries that regulate brain, heart and kidney blood flow. ACE2 converts vasoconstricting angiotensin II into vasodilating angiotensin-(1-7). In brain slices from hamster, which has an ACE2 sequence similar to human ACE2, angiotensin II evoked a small pericyte-mediated capillary constriction via AT1 receptors, but evoked a large constriction when the SARS-CoV-2 receptor binding domain (RBD, original Wuhan variant) was present. A mutated non-binding RBD did not potentiate constriction. A similar RBD-potentiated capillary constriction occurred in human cortical slices, and was evoked in hamster brain slices by pseudotyped virions expressing SARS-CoV-2 spike protein. This constriction reflects an RBD-induced decrease in the conversion of angiotensin II to angiotensin-(1-7) mediated by removal of ACE2 from the cell surface membrane and was mimicked by blocking ACE2. The clinically used drug losartan inhibited the RBD-potentiated constriction. Thus, AT1 receptor blockers could be protective in COVID-19 by preventing pericyte-mediated blood flow reductions in the brain, and perhaps the heart and kidney.
Keywords: SARS-CoV-2; capillary; pericyte.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures

Comment in
-
SARS-CoV-2 targets pericytes to restrict blood flow within the brain.Brain. 2023 Feb 13;146(2):418-420. doi: 10.1093/brain/awac481. Brain. 2023. PMID: 36535909 No abstract available.
Similar articles
-
Enhanced Binding of SARS-CoV-2 Spike Protein to Receptor by Distal Polybasic Cleavage Sites.ACS Nano. 2020 Aug 25;14(8):10616-10623. doi: 10.1021/acsnano.0c04798. Epub 2020 Aug 4. ACS Nano. 2020. PMID: 32806067
-
The pivotal link between ACE2 deficiency and SARS-CoV-2 infection.Eur J Intern Med. 2020 Jun;76:14-20. doi: 10.1016/j.ejim.2020.04.037. Epub 2020 Apr 20. Eur J Intern Med. 2020. PMID: 32336612 Free PMC article. Review.
-
In silico Nigellidine (N. sativa) bind to viral spike/active-sites of ACE1/2, AT1/2 to prevent COVID-19 induced vaso-tumult/vascular-damage/comorbidity.Vascul Pharmacol. 2021 Jun;138:106856. doi: 10.1016/j.vph.2021.106856. Epub 2021 Mar 18. Vascul Pharmacol. 2021. PMID: 33746069 Free PMC article.
-
SARS-CoV-2 deregulates the vascular and immune functions of brain pericytes via Spike protein.Neurobiol Dis. 2021 Dec;161:105561. doi: 10.1016/j.nbd.2021.105561. Epub 2021 Nov 13. Neurobiol Dis. 2021. PMID: 34780863 Free PMC article.
-
Potential use of the S-protein-Angiotensin converting enzyme 2 binding pathway in the treatment of coronavirus disease 2019.Front Public Health. 2022 Nov 28;10:1050034. doi: 10.3389/fpubh.2022.1050034. eCollection 2022. Front Public Health. 2022. PMID: 36518573 Free PMC article. Review.
Cited by
-
Deficiency of fibroblast growth factor 2 promotes contractile phenotype of pericytes in ascending thoracic aortic aneurysm.Am J Physiol Heart Circ Physiol. 2025 May 1;328(5):H1130-H1143. doi: 10.1152/ajpheart.00834.2024. Epub 2025 Apr 11. Am J Physiol Heart Circ Physiol. 2025. PMID: 40214073 Free PMC article.
-
Moderate, Little, or No Improvements in Neurobehavioral Symptoms among Individuals with Long COVID: A 34-Country Retrospective Study.Int J Environ Res Public Health. 2022 Oct 2;19(19):12593. doi: 10.3390/ijerph191912593. Int J Environ Res Public Health. 2022. PMID: 36231893 Free PMC article.
-
Fluoxetine plus lithium for treatment of mental health impairment in Long Covid.Discov Ment Health. 2023;3(1):1. doi: 10.1007/s44192-022-00027-w. Epub 2023 Jan 3. Discov Ment Health. 2023. PMID: 36618714 Free PMC article. Review.
-
Unraveling the SARS-CoV-2 spike protein long-term effect on neuro-PASC.Front Cell Neurosci. 2024 Dec 18;18:1481963. doi: 10.3389/fncel.2024.1481963. eCollection 2024. Front Cell Neurosci. 2024. PMID: 39744674 Free PMC article.
-
Diabetes as a Pancreatic Microvascular Disease-A Pericytic Perspective.J Histochem Cytochem. 2024 Mar;72(3):131-148. doi: 10.1369/00221554241236535. Epub 2024 Mar 7. J Histochem Cytochem. 2024. PMID: 38454609 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
