

Treatment strategy on traumatic mid-lumbar spondyloptosis with concomitant multiple injuries: A case report and literature review
- PMID: 35868949
- PMCID: PMC9912182
- DOI: 10.1016/j.cjtee.2022.06.006
Treatment strategy on traumatic mid-lumbar spondyloptosis with concomitant multiple injuries: A case report and literature review
Abstract
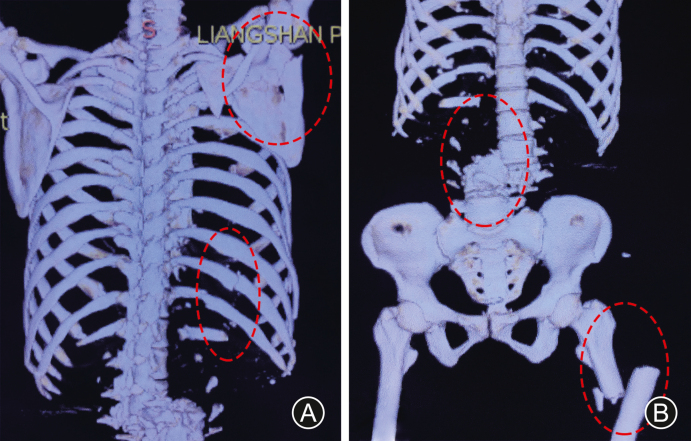
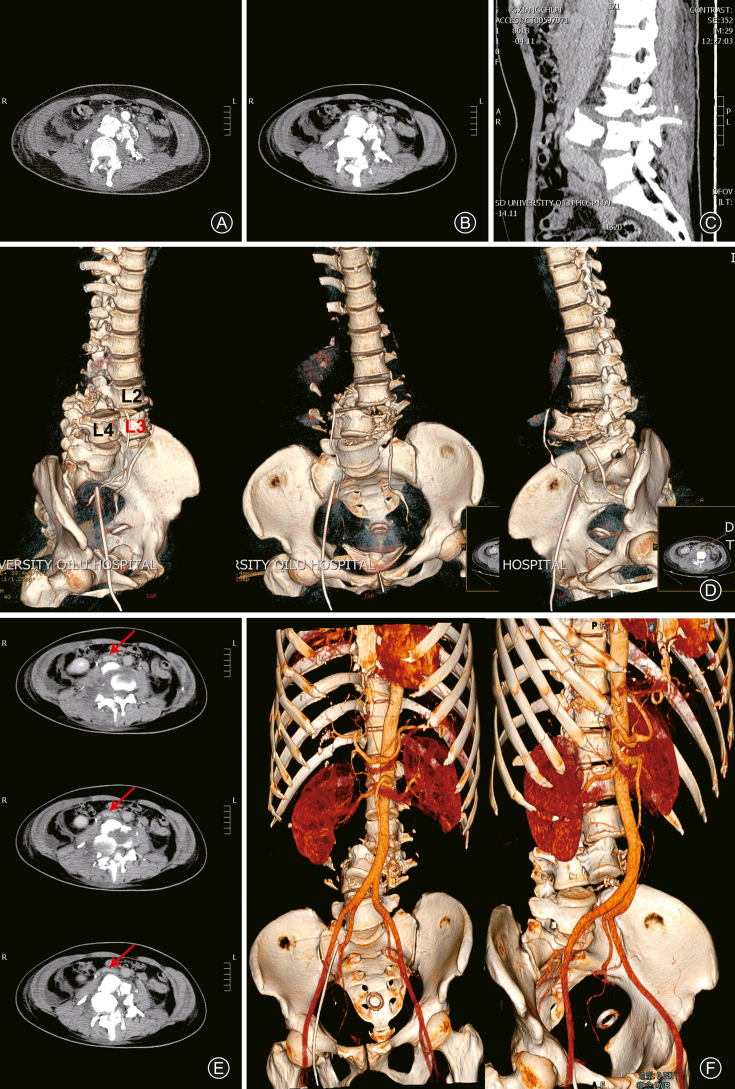
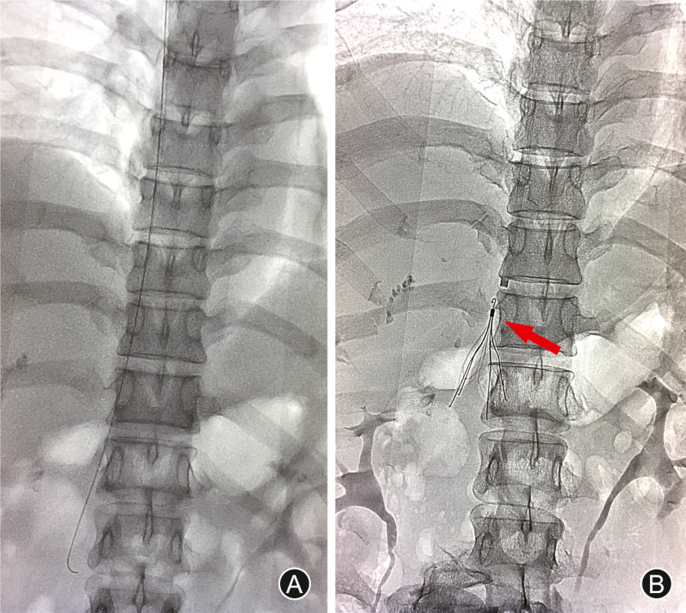
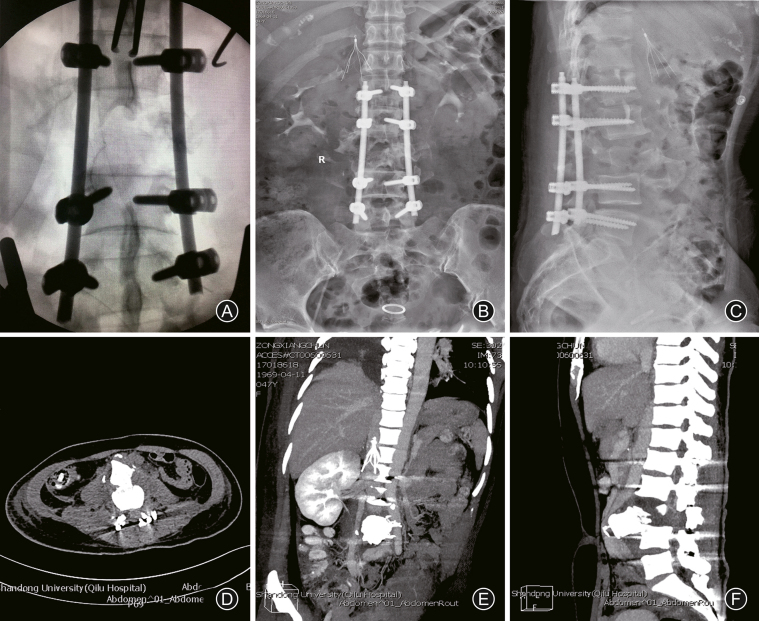
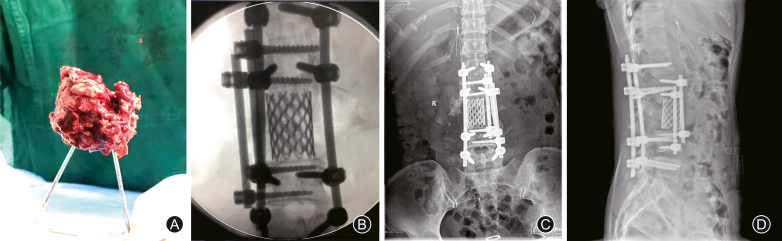
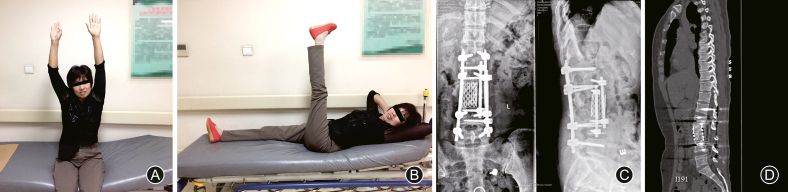
Spondyloptosis in the clinic is rarely reported. We herein present a 47-year-old female, who suffered from a crush injury directly by a heavy cylindrical object from the lateral side. She was diagnosed to have traumatic L3 spondyloptosis with multiple traumas. Staged surgical procedures were conducted and a three-year follow-up was obtained. Eventually, normal spinal alignment was restored, and neurological deficits were gradually improved. At three years follow-up, the motor strength scores and function of the sphincters were incompletely improved. Previously published reports on traumatic lumbar spondyloptosis were reviewed and several critical points for management of this severe type of spinal injury were proposed. First, thoracolumbar and lumbosacral junction were mostly predilection sites. Second, numerous patients involving traumatic lumbar spondyloptosis were achieved to American Spinal Injury Association grade A. Third, lumbar spondyloptosis was commonly coupling with cauda equina injury. Finally, the outcomes were still with poorly prognosis and recovery of patients was correlation to spondyloptosis severity. Based on this case report and literatures review, we highlighted that the spinal alignment restoration relying on staged operations and following rehabilitation hereof are both important once facing with multiple traumas. Furthermore, we suggested to perform routine CT angiography during lumbar spondyloptosis to justify whether there are large vessel compression or injury.
Keywords: American Spinal Injury Association; Fracture dislocation; Lumbar spine; Multiple trauma; Spondyloptosis.
Copyright © 2022 Chinese Medical Association. Production and hosting by Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Mid-lumbar traumatic spondyloptosis without neurological deficit: A case report and literature review.Medicine (Baltimore). 2020 Mar;99(12):e19578. doi: 10.1097/MD.0000000000019578. Medicine (Baltimore). 2020. PMID: 32195971 Free PMC article. Review.
-
Traumatic spondyloptosis: a series of 20 patients.J Neurosurg Spine. 2015 Jun;22(6):647-52. doi: 10.3171/2014.10.SPINE1440. Epub 2015 Mar 13. J Neurosurg Spine. 2015. PMID: 25768668
-
Traumatic spondyloptosis of the thoracolumbar spine.J Neurosurg Spine. 2008 Aug;9(2):145-51. doi: 10.3171/SPI/2008/9/8/145. J Neurosurg Spine. 2008. PMID: 18764746
-
Traumatic spondyloptosis of the lumbar spine: a case report.J Med Case Rep. 2014 Dec 21;8:453. doi: 10.1186/1752-1947-8-453. J Med Case Rep. 2014. PMID: 25528055 Free PMC article.
-
Traumatic lumbosacral spondyloptosis treated five months after injury occurrence: a case report.Spine (Phila Pa 1976). 2012 Oct 15;37(22):E1410-4. doi: 10.1097/BRS.0b013e318268c08a. Spine (Phila Pa 1976). 2012. PMID: 22805340 Review.
Cited by
-
Case report: Traumatic lumbosacral spondyloptosis with locked L5 inferior articular process.Front Surg. 2023 Jun 26;10:1174169. doi: 10.3389/fsurg.2023.1174169. eCollection 2023. Front Surg. 2023. PMID: 37435471 Free PMC article.
-
Acute Traumatic Lumbar Spondyloptosis with Complete Neurological Deficit: A Case Report and Literature Review.J Orthop Case Rep. 2025 Apr;15(4):180-185. doi: 10.13107/jocr.2025.v15.i04.5492. J Orthop Case Rep. 2025. PMID: 40212502 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical