

Face mediated human-robot interaction for remote medical examination
- PMID: 35869154
- PMCID: PMC9307637
- DOI: 10.1038/s41598-022-16643-z
Face mediated human-robot interaction for remote medical examination
Abstract
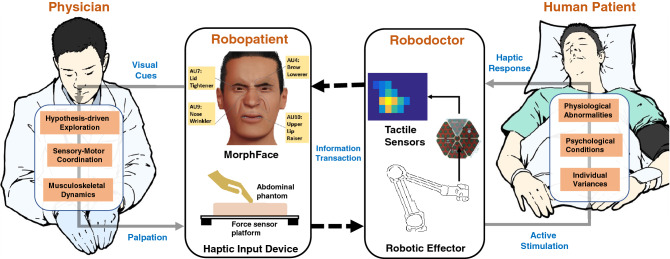
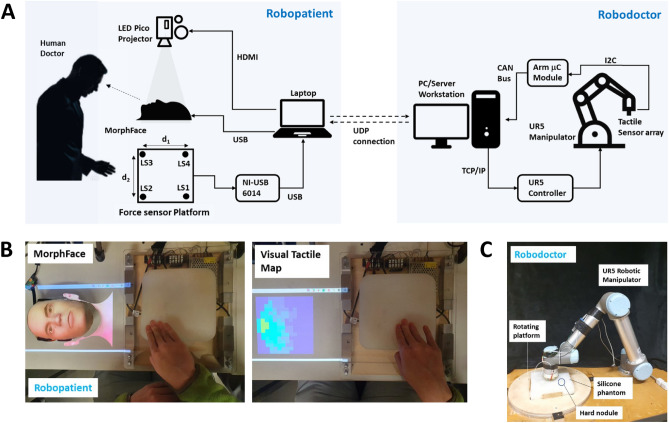
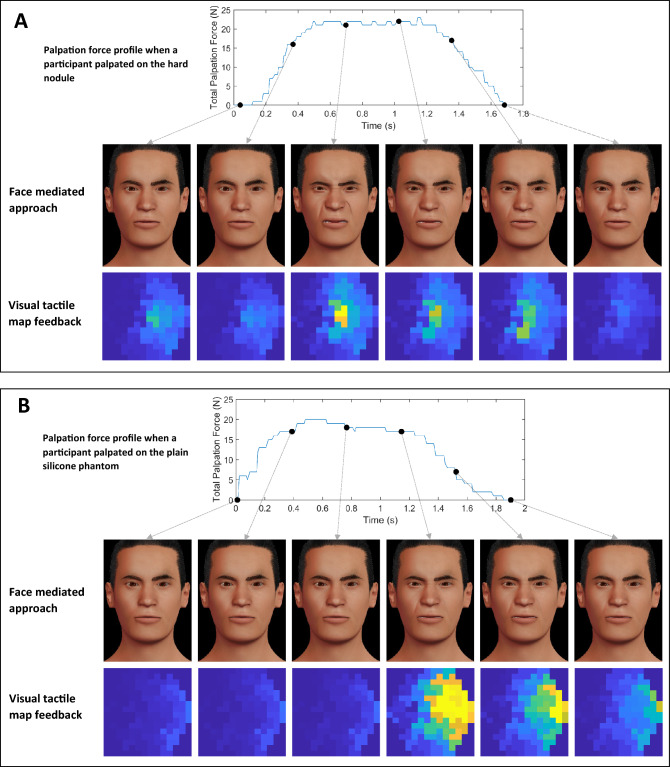
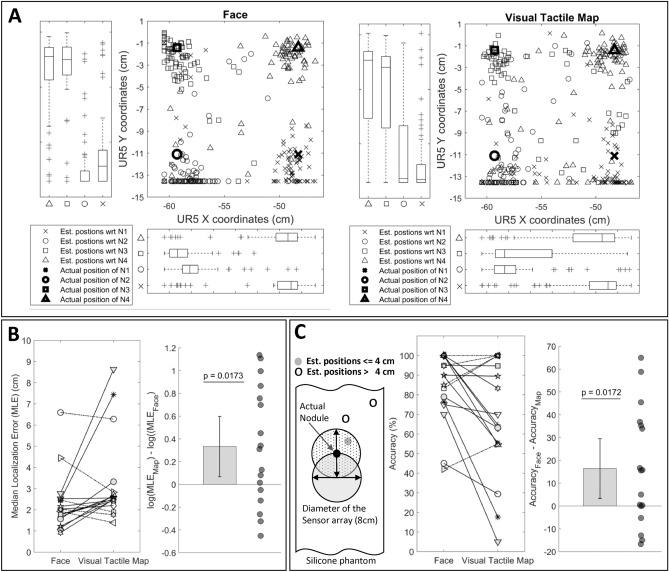
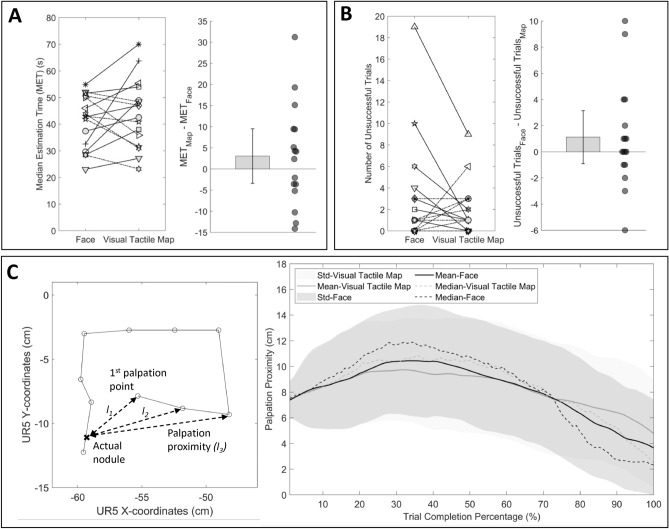
Realtime visual feedback from consequences of actions is useful for future safety-critical human-robot interaction applications such as remote physical examination of patients. Given multiple formats to present visual feedback, using face as feedback for mediating human-robot interaction in remote examination remains understudied. Here we describe a face mediated human-robot interaction approach for remote palpation. It builds upon a robodoctor-robopatient platform where user can palpate on the robopatient to remotely control the robodoctor to diagnose a patient. A tactile sensor array mounted on the end effector of the robodoctor measures the haptic response of the patient under diagnosis and transfers it to the robopatient to render pain facial expressions in response to palpation forces. We compare this approach against a direct presentation of tactile sensor data in a visual tactile map. As feedback, the former has the advantage of recruiting advanced human capabilities to decode expressions on a human face whereas the later has the advantage of being able to present details such as intensity and spatial information of palpation. In a user study, we compare these two approaches in a teleoperated palpation task to find the hard nodule embedded in the remote abdominal phantom. We show that the face mediated human-robot interaction approach leads to statistically significant improvements in localizing the hard nodule without compromising the nodule position estimation time. We highlight the inherent power of facial expressions as communicative signals to enhance the utility and effectiveness of human-robot interaction in remote medical examinations.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Birdwhistell RL. Kinesics and Context: Essays on Body Motion Communication. Allen Lane The Penguin Press; 1971.
-
- Mitchell A, Drake R, Vogl A. Gray’s Anatomy for Students. 3. Elsevier; 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
