

Limited generalizability of single deep neural network for surgical instrument segmentation in different surgical environments
- PMID: 35869249
- PMCID: PMC9307578
- DOI: 10.1038/s41598-022-16923-8
Limited generalizability of single deep neural network for surgical instrument segmentation in different surgical environments
Abstract
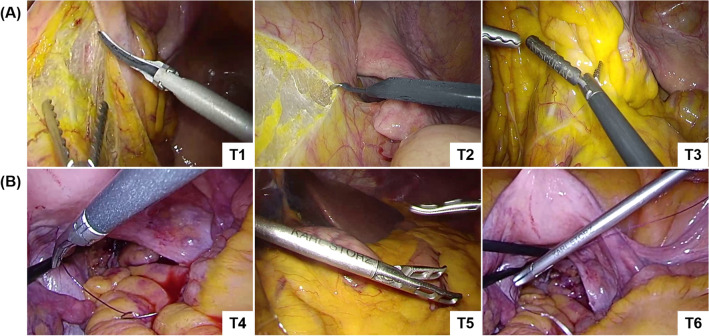
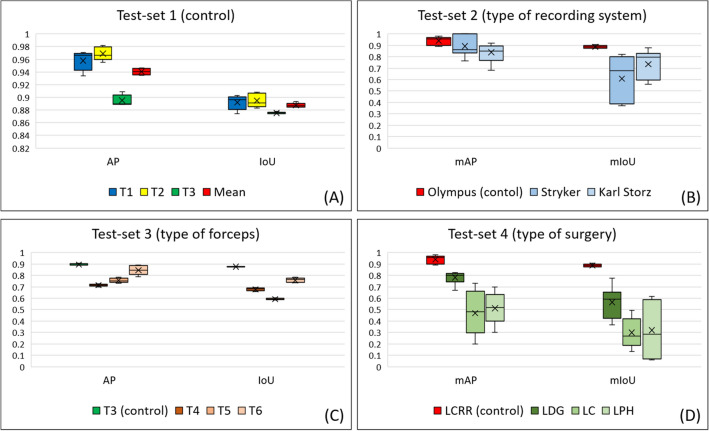
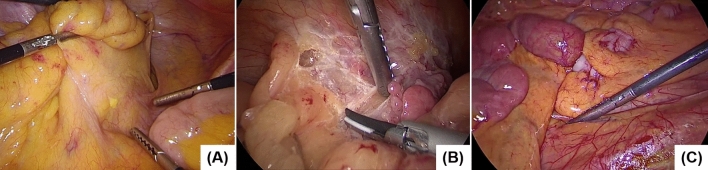
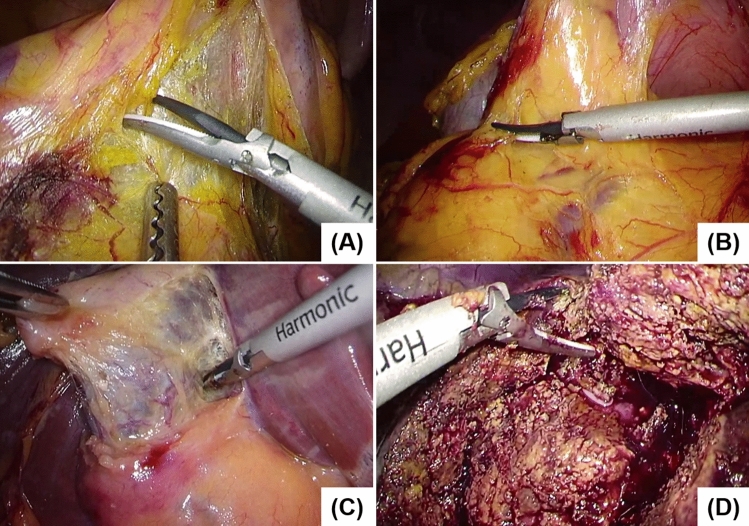
Clarifying the generalizability of deep-learning-based surgical-instrument segmentation networks in diverse surgical environments is important in recognizing the challenges of overfitting in surgical-device development. This study comprehensively evaluated deep neural network generalizability for surgical instrument segmentation using 5238 images randomly extracted from 128 intraoperative videos. The video dataset contained 112 laparoscopic colorectal resection, 5 laparoscopic distal gastrectomy, 5 laparoscopic cholecystectomy, and 6 laparoscopic partial hepatectomy cases. Deep-learning-based surgical-instrument segmentation was performed for test sets with (1) the same conditions as the training set; (2) the same recognition target surgical instrument and surgery type but different laparoscopic recording systems; (3) the same laparoscopic recording system and surgery type but slightly different recognition target laparoscopic surgical forceps; (4) the same laparoscopic recording system and recognition target surgical instrument but different surgery types. The mean average precision and mean intersection over union for test sets 1, 2, 3, and 4 were 0.941 and 0.887, 0.866 and 0.671, 0.772 and 0.676, and 0.588 and 0.395, respectively. Therefore, the recognition accuracy decreased even under slightly different conditions. The results of this study reveal the limited generalizability of deep neural networks in the field of surgical artificial intelligence and caution against deep-learning-based biased datasets and models.Trial Registration Number: 2020-315, date of registration: October 5, 2020.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
