

Vancomycin area under the curve versus trough only guided dosing and the risk of acute kidney injury: Systematic review and meta-analysis
- PMID: 35869689
- PMCID: PMC9481691
- DOI: 10.1002/phar.2722
Vancomycin area under the curve versus trough only guided dosing and the risk of acute kidney injury: Systematic review and meta-analysis
Abstract
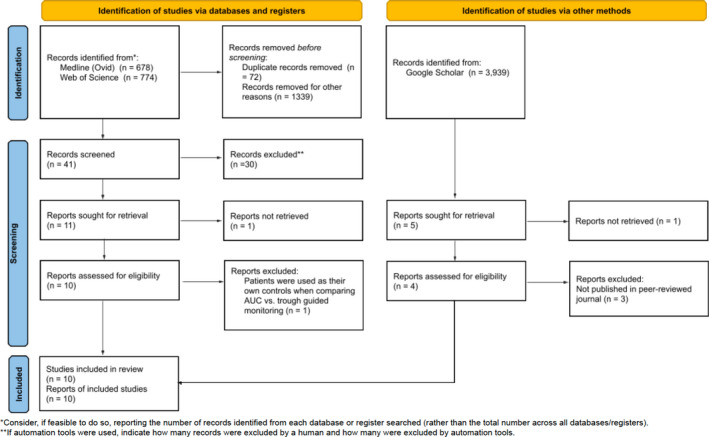
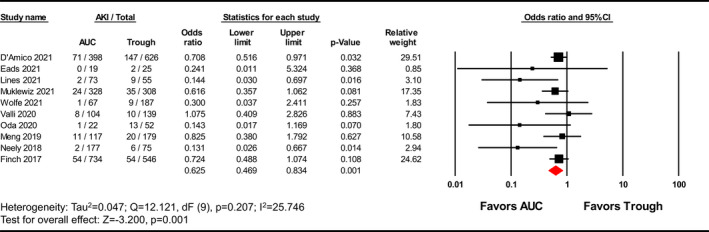
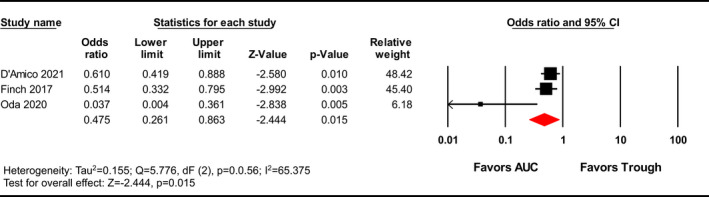
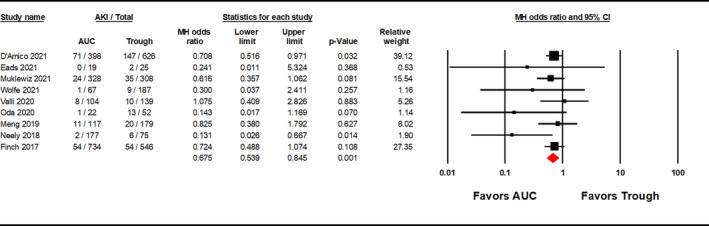
Vancomycin is commonly used to treat methicillin-resistant Staphylococcus aureus infections and is known to cause nephrotoxicity. Previous Vancomycin Consensus Guidelines recommended targeting trough concentrations but the 2020 Guidelines suggest monitoring vancomycin area under the curve (AUC) given the reduced risk of acute kidney injury (AKI) at similar levels of efficacy. This meta-analysis compares vancomycin-induced AKI incidence using AUC-guided dosing strategies versus trough-based monitoring. Literature was queried from Medline (Ovid), Web of Science, and Google Scholar from database inception through November 5, 2021. Interventional or observational studies reporting the incidence of vancomycin-induced AKI between AUC- and trough-guided dosing strategies were included. In the primary analysis, the Vancomycin Consensus Guidelines definition for AKI was used if reported; otherwise, the Risk, Injury, and Failure; and Loss, and End-stage kidney disease (RIFLE) or Kidney Disease Improving Global Outcomes (KDIGO) definitions were used. The incidence of nephrotoxicity was evaluated between the two strategies using a Mantel-Haenszel random-effects model, and odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Subgroup analyses for adjusted ORs and AKI definitions were performed. Heterogeneity was identified using Cochrane's Q test and I2 statistics. A total of 10 studies with 4231 patients were included. AUC-guided dosing strategies were associated with significantly less vancomycin-induced AKI than trough-guided strategies [OR 0.625, 95% CI (0.469-0.834), p = 0.001; I2 = 25.476]. A subgroup analysis of three studies reporting adjusted ORs yielded similar results [OR 0.475, 95% CI (0.261-0.863), p = 0.015]. Stratification by AKI definition showed a significant reduction in AKI with the Vancomycin Consensus Guidelines definition [OR 0.552, 95% CI (0.341-0.894), p = 0.016] but failed to find significance in the alternative definitions. Area under the curve-guided dosing strategies are associated with a lower incidence of vancomycin-induced AKI versus trough-guided dosing strategies (GRADE, low). Limitations included the variety of AKI definitions and the potential for confounding bias.
Keywords: acute kidney injury; area under the curve; nephrotoxicity; trough; vancomycin.
© 2022 The Authors. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy published by Wiley Periodicals LLC on behalf of Pharmacotherapy Publications, Inc.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

Similar articles
-
Impact of model-informed precision dosing on achievement of vancomycin exposure targets in pediatric patients with cystic fibrosis.Pharmacotherapy. 2023 Oct;43(10):1007-1014. doi: 10.1002/phar.2845. Epub 2023 Jul 11. Pharmacotherapy. 2023. PMID: 37401162
-
A Multicenter, Retrospective Outcome Analysis of Vancomycin Area Under the Curve Versus Trough-Based Dosing Strategies in Patients With Burn OR Inhalational Injuries (MONITOR).J Burn Care Res. 2024 Nov 14;45(6):1383-1389. doi: 10.1093/jbcr/irae109. J Burn Care Res. 2024. PMID: 38900835
-
Evaluating the Nephrotoxicity of Area-under-the-Curve-Based Dosing of Vancomycin with Concomitant Antipseudomonal Beta-Lactam Antibiotics: A Systematic Review and Meta-Analysis.Medicina (Kaunas). 2023 Mar 31;59(4):691. doi: 10.3390/medicina59040691. Medicina (Kaunas). 2023. PMID: 37109649 Free PMC article.
-
A Large Cohort Study to Identify Risk Factors of Acute Kidney Injury in Pediatric Patients Undergoing Intravenous Vancomycin Therapy.Pharmacotherapy. 2025 Aug;45(8):504-511. doi: 10.1002/phar.70044. Epub 2025 Jul 26. Pharmacotherapy. 2025. PMID: 40715988 Free PMC article.
-
The Relationship Between Vancomycin Trough Concentrations and AUC/MIC Ratios in Pediatric Patients: A Qualitative Systematic Review.Paediatr Drugs. 2018 Apr;20(2):153-164. doi: 10.1007/s40272-018-0282-4. Paediatr Drugs. 2018. PMID: 29344778
Cited by
-
Impact of Pharmacist-Led Multidisciplinary Team to Attain Targeted Vancomycin Area under the Curved Monitoring in a Tertiary Care Center in Thailand.Antibiotics (Basel). 2023 Feb 11;12(2):374. doi: 10.3390/antibiotics12020374. Antibiotics (Basel). 2023. PMID: 36830284 Free PMC article.
-
Systematic review of efficacy, safety and pharmacokinetics of intravenous and intraventricular vancomycin for central nervous system infections.Front Pharmacol. 2022 Nov 18;13:1056148. doi: 10.3389/fphar.2022.1056148. eCollection 2022. Front Pharmacol. 2022. PMID: 36467047 Free PMC article. Review.
-
Vancomycin Area under the Concentration-Time Curve Estimation Using Bayesian Modeling versus First-Order Pharmacokinetic Equations: A Quasi-Experimental Study.Antibiotics (Basel). 2022 Sep 13;11(9):1239. doi: 10.3390/antibiotics11091239. Antibiotics (Basel). 2022. PMID: 36140021 Free PMC article.
-
Association between trough serum vancomycin concentration and vancomycin-associated acute kidney injury and 30-day mortality in critically ill elderly adults.BMC Infect Dis. 2024 Mar 20;24(1):330. doi: 10.1186/s12879-024-09227-x. BMC Infect Dis. 2024. PMID: 38509460 Free PMC article.
-
Impact of the First Twenty-Four-Hour Area Under the Concentration-Time Curve/Minimum Inhibitory Concentration of Vancomycin on Treatment Outcomes in Patients With Methicillin-Resistant Staphylococcus aureus Bacteremia.J Clin Med Res. 2024 Aug;16(7-8):325-334. doi: 10.14740/jocmr5238. Epub 2024 Aug 10. J Clin Med Res. 2024. PMID: 39206105 Free PMC article.
References
-
- Patel S, Preuss CV, Bernice F. Vancomycin. In: StatPearls. StatPearls Publishing. Copyright © 2022, StatPearls Publishing LLC; 2022.
-
- Association AH . Fast facts on U.S. hospitals; 2022. Accessed July 1, 2022. https://www.aha.org/statistics/fast‐facts‐us‐hospitals
-
- Rybak MJ, Le J, Lodise TP, et al. Executive summary: therapeutic monitoring of vancomycin for serious methicillin‐resistant Staphylococcus aureus infections: a revised consensus guideline and review of the American Society of Health‐System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Pharmacotherapy. 2020;4:363‐367. - PubMed
-
- Patel N, Huang D, Lodise T. Potential for cost saving with iclaprim owing to avoidance of vancomycin‐associated acute kidney injury in hospitalized patients with acute bacterial skin and skin structure infections. Clin Drug Investig. 2018;10:935‐943. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
