

Functional outcomes in patient specific instrumentation vs. conventional instrumentation for total knee arthroplasty; a systematic review and meta-analysis of prospective studies
- PMID: 35870913
- PMCID: PMC9308296
- DOI: 10.1186/s12891-022-05620-2
Functional outcomes in patient specific instrumentation vs. conventional instrumentation for total knee arthroplasty; a systematic review and meta-analysis of prospective studies
Abstract
Background: Total Knee Arthroplasty (TKA) is an established surgical option for knee osteoarthritis (OA). There are varying perceptions of the most suitable surgical technique for making bone cuts in TKA. Conventional Instrumentation (CI) uses generic cutting guides (extra- and intra-medullary) for TKA; however, patient specific instrumentation (PSI) has become a popular alternative amongst surgeons.
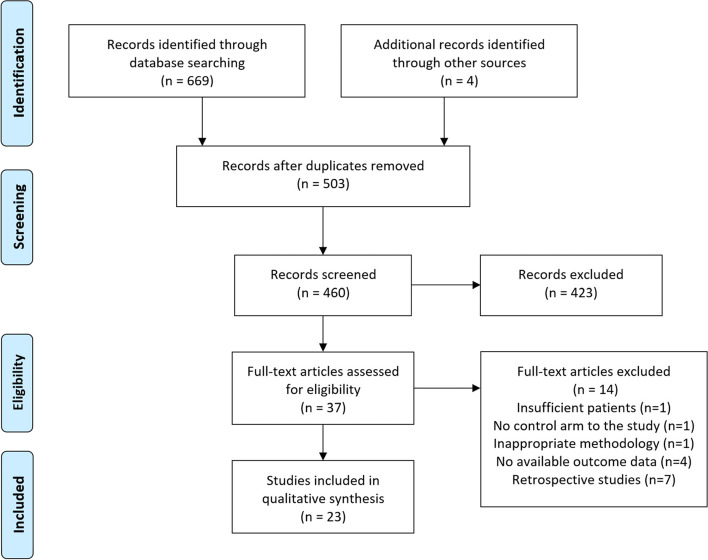
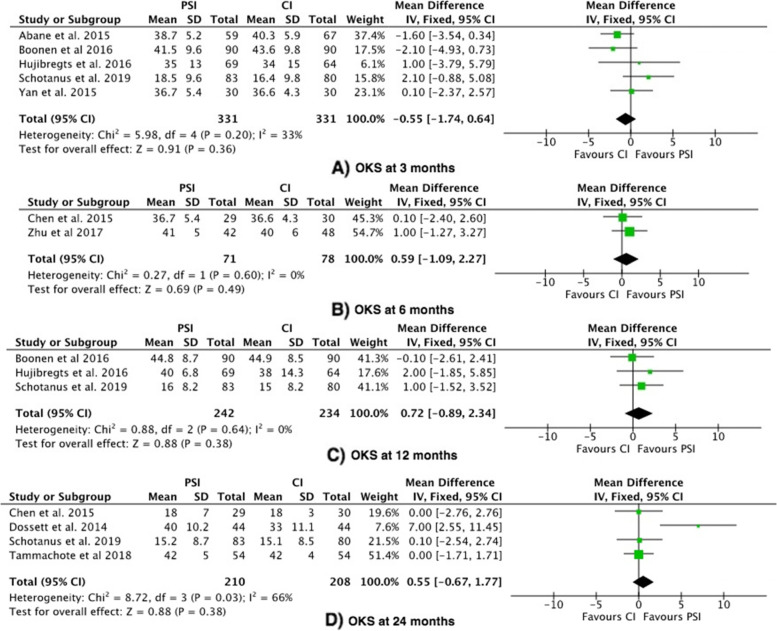
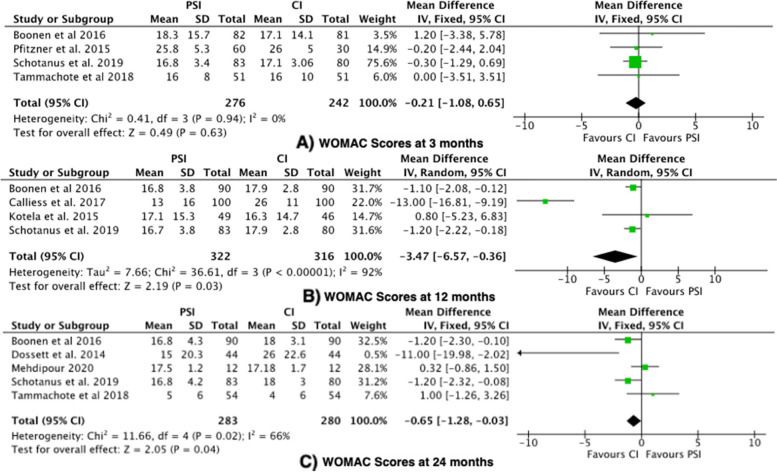
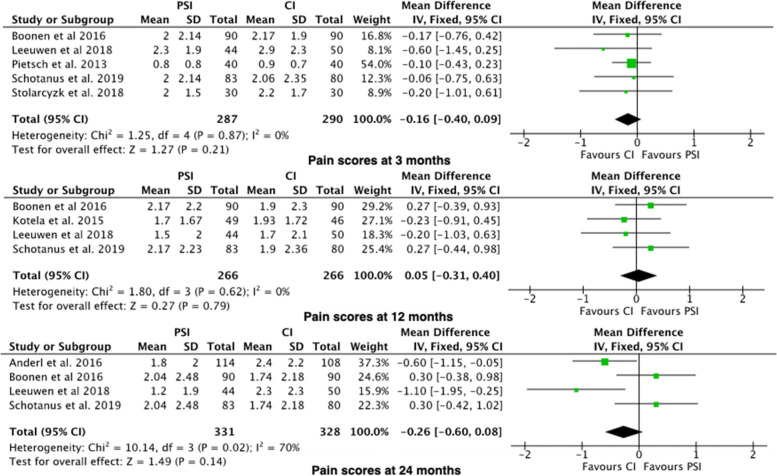
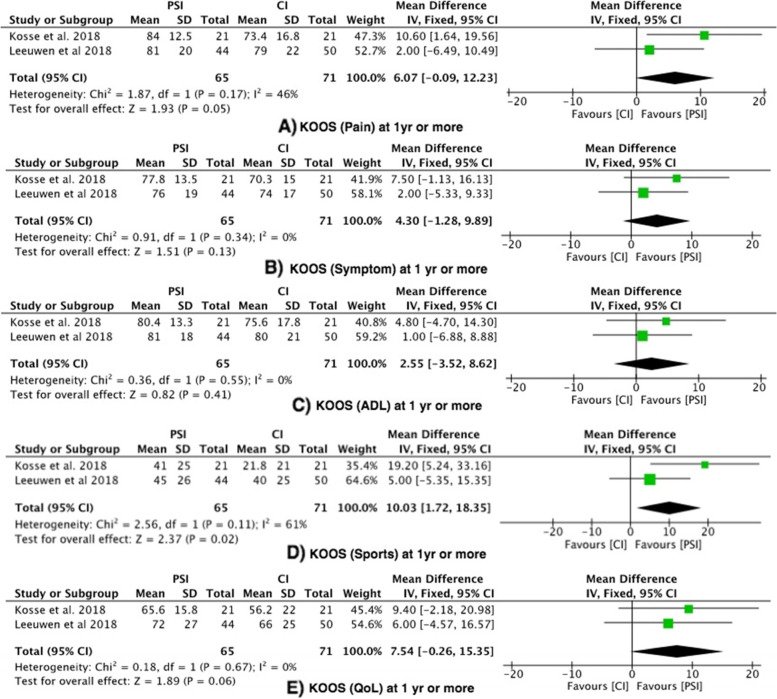
Methods: A literature search of electronic databases Embase, Medline and registry platform portals was conducted on the 16th May 2021. The search was performed using a predesigned search strategy. Eligible studies were critically appraised for methodological quality. The primary outcome measure was Knee Society Function Score. Functional scores were also collected for the secondary outcome measures: Oxford Knee Score (OKS), Western Ontario and McMaster Universities Arthritis Index (WOMAC), Knee Injury and Osteoarthritis Outcome Score (KOOS) and Visual Analog Scale (VAS) for pain. Review Manager 5.3 was used for all data synthesis and analysis.
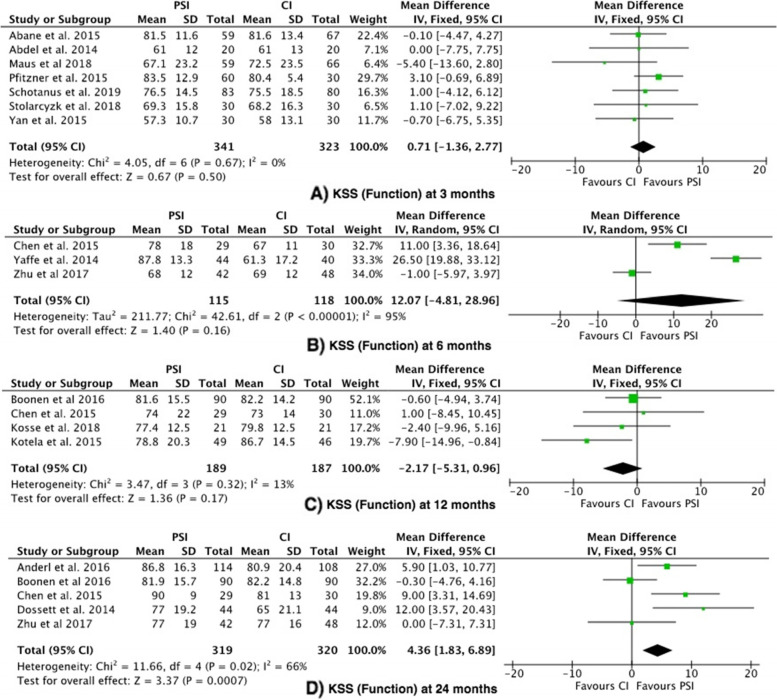
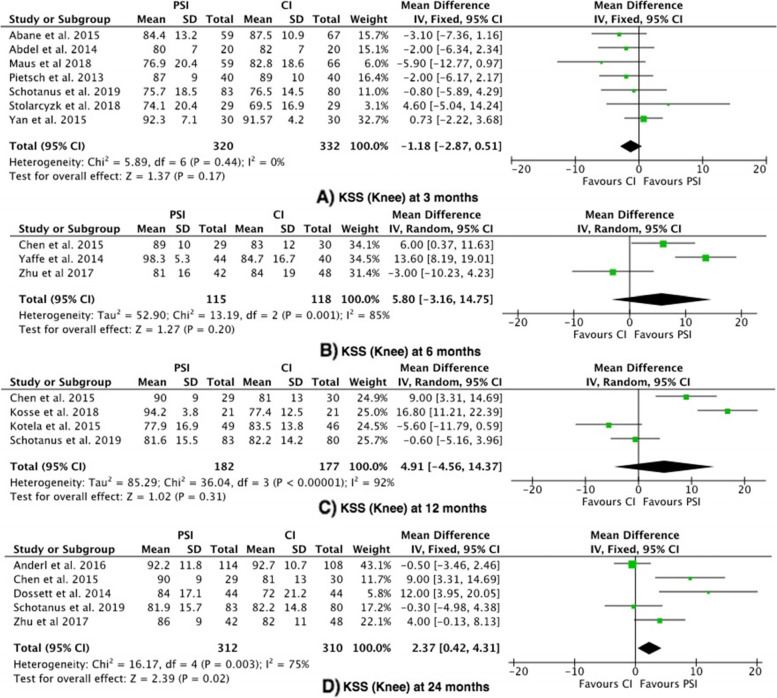
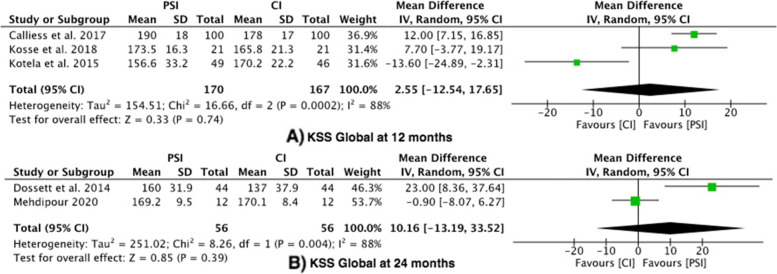
Results: There is no conclusive evidence in the literature to suggest that PSI or CI instrumentation is better for functional outcomes. 23 studies were identified for inclusion in this study. Twenty-two studies (18 randomised controlled trials and 4 prospective studies) were included in the meta analysis, with a total of 2277 total knee arthroplasties. There were 1154 PSI TKA and 1123 CI TKA. The majority of outcomes at 3-months, 6-months and 12 show no statistical difference. There was statistical significance at 24 months in favour of PSI group for KSS function (mean difference 4.36, 95% confidence interval 1.83-6.89). The mean difference did not exceed the MCID of 6.4. KSS knee scores demonstrated statistical significance at 24 months (mean difference 2.37, 95% confidence interval (CI) 0.42-4.31), with a MCID of 5.9. WOMAC scores were found to be statistically significant favouring PSI group at 12 months (mean difference -3.47, 95% confidence interval (CI) -6.57- -0.36) and 24 months (mean difference -0.65, 95% confidence interval (CI) -1.28--0.03), with high level of bias noted in the studies and a MCID of 10.
Conclusions: This meta-analysis of level 1 and level 2 evidence shows there is no clinical difference when comparing PSI and CI KSS function scores for TKA at definitive post operative time points (3 months, 6 months, 12 months and 24 months). Within the secondary outcomes for this study, there was no clinical difference between PSI and CI for TKA. Although there was no clinical difference between PSI and CI for TKA, there was statistical significance noted at 24 months in favour of PSI compared to CI for TKA when considering KSS function, KSS knee scores and WOMAC scores. Studies included in this meta-analysis were of limited cohort size and prospective studies were prone to methodological bias. The current literature is limited and insufficiently robust to make explicit conclusions and therefore further high-powered robust RCTs are required at specific time points.
Keywords: Meta-analysis; Patient-Specific; Total Knee Arthroplasty.
© 2022. The Author(s).
Conflict of interest statement
The authors whose names are listed immediately below certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Figures
Similar articles
-
Outcome of kinematic alignment using patient-specific instrumentation versus mechanical alignment in TKA: a meta-analysis and subgroup analysis of randomised trials.Arch Orthop Trauma Surg. 2018 Sep;138(9):1293-1303. doi: 10.1007/s00402-018-2988-8. Epub 2018 Jun 30. Arch Orthop Trauma Surg. 2018. PMID: 29961093
-
Patient-specific instrumentation improved mechanical alignment, while early clinical outcome was comparable to conventional instrumentation in TKA.Knee Surg Sports Traumatol Arthrosc. 2016 Jan;24(1):102-11. doi: 10.1007/s00167-014-3345-2. Epub 2014 Oct 19. Knee Surg Sports Traumatol Arthrosc. 2016. PMID: 25326759
-
Total knee arthroplasty using patient-specific instrumentation for osteoarthritis of the knee: a meta-analysis.BMC Musculoskelet Disord. 2019 Nov 23;20(1):561. doi: 10.1186/s12891-019-2940-2. BMC Musculoskelet Disord. 2019. PMID: 31759392 Free PMC article.
-
A Meta-analysis of Functional Outcomes in Patient-Specific Instrumented Knee Arthroplasty.J Knee Surg. 2017 Sep;30(7):668-674. doi: 10.1055/s-0036-1593869. Epub 2016 Dec 1. J Knee Surg. 2017. PMID: 27907935
-
Medial stabilised total knee arthroplasty achieves comparable clinical outcomes when compared to other TKA designs: a systematic review and meta-analysis of the current literature.Knee Surg Sports Traumatol Arthrosc. 2022 Feb;30(2):638-651. doi: 10.1007/s00167-020-06358-x. Epub 2020 Nov 27. Knee Surg Sports Traumatol Arthrosc. 2022. PMID: 33247352 Free PMC article.
Cited by
-
Patient Specific Instruments and Patient Individual Implants-A Narrative Review.J Pers Med. 2023 Feb 27;13(3):426. doi: 10.3390/jpm13030426. J Pers Med. 2023. PMID: 36983609 Free PMC article. Review.
-
[New technologies in total knee arthroplasty : Current concepts and personalized treatment strategies].Orthopadie (Heidelb). 2025 Mar;54(3):190-198. doi: 10.1007/s00132-025-04618-7. Epub 2025 Feb 17. Orthopadie (Heidelb). 2025. PMID: 39961906 Review. German.
-
Custom total knee arthroplasty combined with personalised alignment grants 94% patient satisfaction at minimum follow-up of 2 years.Knee Surg Sports Traumatol Arthrosc. 2023 Apr;31(4):1276-1283. doi: 10.1007/s00167-023-07318-x. Epub 2023 Jan 19. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 36656348
-
Flexion contracture can cause component mismatch in the Prophecy® preoperative patient-specific instrumentation for Evolution® medial-pivot knee system.SICOT J. 2024;10:12. doi: 10.1051/sicotj/2024009. Epub 2024 Apr 9. SICOT J. 2024. PMID: 38592306 Free PMC article.
-
Evaluation of component alignment in total knee arthroplasty using patient-specific instrumentation versus conventional guides: a retrospective study.SICOT J. 2025;11:44. doi: 10.1051/sicotj/2025044. Epub 2025 Aug 4. SICOT J. 2025. PMID: 40758900 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
