

Clinical utility of the BIWACO score for patients with atrial fibrillation after percutaneous coronary intervention
- PMID: 35871206
- PMCID: PMC9810676
- DOI: 10.1007/s00380-022-02128-6
Clinical utility of the BIWACO score for patients with atrial fibrillation after percutaneous coronary intervention
Abstract
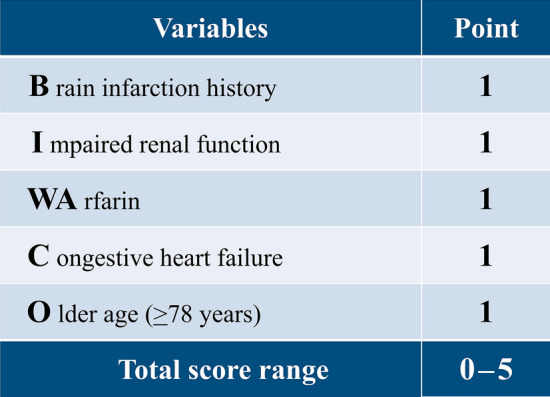
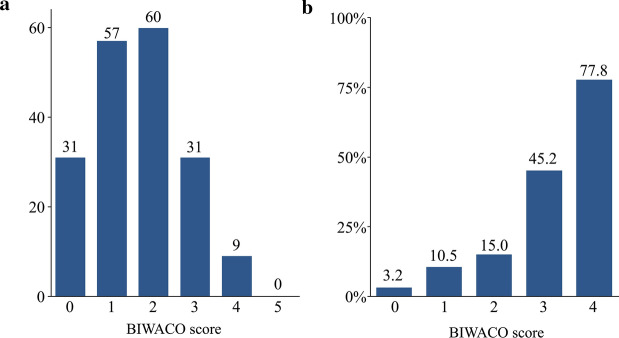
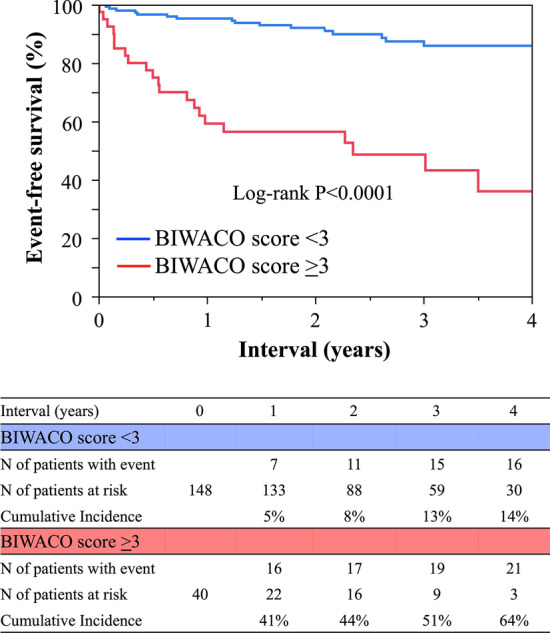
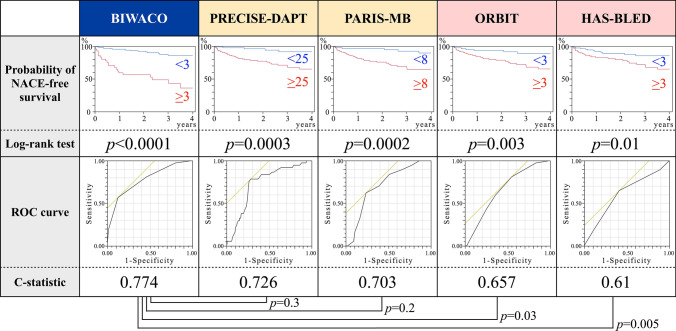
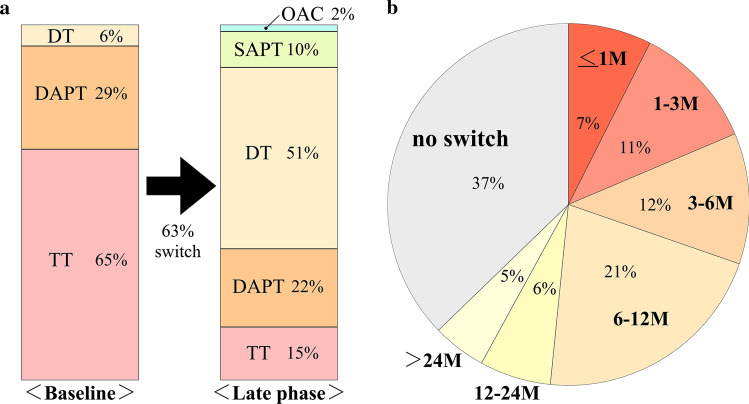
No predictive clinical risk scores for net adverse clinical events (NACE) have been developed for patients with atrial fibrillation (AF) after percutaneous coronary intervention (PCI). We evaluated NACE to develop clinically applicable risk-stratification scores in the Bleeding and thrombotic risk evaluation In patients With Atrial fibrillation under COronary intervention (BIWACO) study, a multicenter survey which has enrolled a total of 7837 patients. We also investigated the current status and time trends for the use of antithrombotic drugs. A total of 188 AF patients who had received PCI were examined. At discharge, 65% of patients were prescribed a triple therapy (TT), 6% were prescribed a dual therapy, the remaining 29% of patients received dual-antiplatelet therapy. After 4 years, the fraction of patients continuing TT decreased by 15%, whereas oral anticoagulant alone was only 2% of patients. NACE developed in 20% of patients, resulting in death in 5% of the patients, and the remaining 13% experienced bleeding events. We developed risk scores for NACE comprising the five strongest predictive items, which we designated BIWACO scores. The area under the curve was 0.774 for NACE. Our study explored the differences in treatment practices and guideline recommendations for antithrombotic therapy. We concluded that our BIWACO score is useful for predicting clinical outcomes in AF-patients after PCI.
Keywords: Anticoagulants; Atrial fibrillation; Percutaneous coronary intervention; Risk score.
© 2022. The Author(s).
Conflict of interest statement
The authors have no disclosures to report.
Figures

References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Després JP, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, Jiménez MC, Judd SE, Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Magid DJ, McGuire DK, Mohler ER 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Rosamond W, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Woo D, Yeh RW, Turner MB (2016) American Heart Association Statistics Committee; Stroke statistics Subcommittee. executive summary: heart disease and stroke statistics 2016 Update: A Report From the American Heart Association. Circulation 133(4):447-454
-
- Nieuwlaat R, Capucci A, Camm AJ, Olsson SB, Andresen D, Davies DW, Cobbe S, Breithardt G, Le Heuzey JY, Prins MH, Lévy S, Crijns HJ. Atrial fibrillation management: a prospective survey in ESC member countries: the Euro Heart Survey on Atrial Fibrillation. Eur Heart J. 2005;26(22):2422–2434. doi: 10.1093/eurheartj/ehi505. - DOI - PubMed
-
- Choi HI, Ahn JM, Kang SH, Lee PH, Kang SJ, Lee SW, Kim YH, Lee CW, Park SW, Park DW, Park SJ. Prevalence, management, and long-term (6-year) outcomes of atrial fibrillation among patients receiving drug-eluting coronary stents. JACC Cardiovasc Interv. 2017;10(11):1075–1085. doi: 10.1016/j.jcin.2017.02.028. - DOI - PubMed
-
- Lopes RD, Hong H, Harskamp RE, Bhatt DL, Mehran R, Cannon CP, Granger CB, Verheugt FWA, Li J, Ten Berg JM, Sarafoff N, Gibson CM, Alexander JH. Safety and efficacy of antithrombotic strategies in patients with atrial fibrillation undergoing percutaneous coronary intervention: a network meta-analysis of randomized controlled trials. JAMA Cardiol. 2019;4(8):747–755. doi: 10.1001/jamacardio.2019.1880. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
