

Factors Affecting Domiciliary Non-Invasive Ventilation Compliance
- PMID: 35871430
- PMCID: PMC9360075
- DOI: 10.1007/s00408-022-00557-8
Factors Affecting Domiciliary Non-Invasive Ventilation Compliance
Abstract
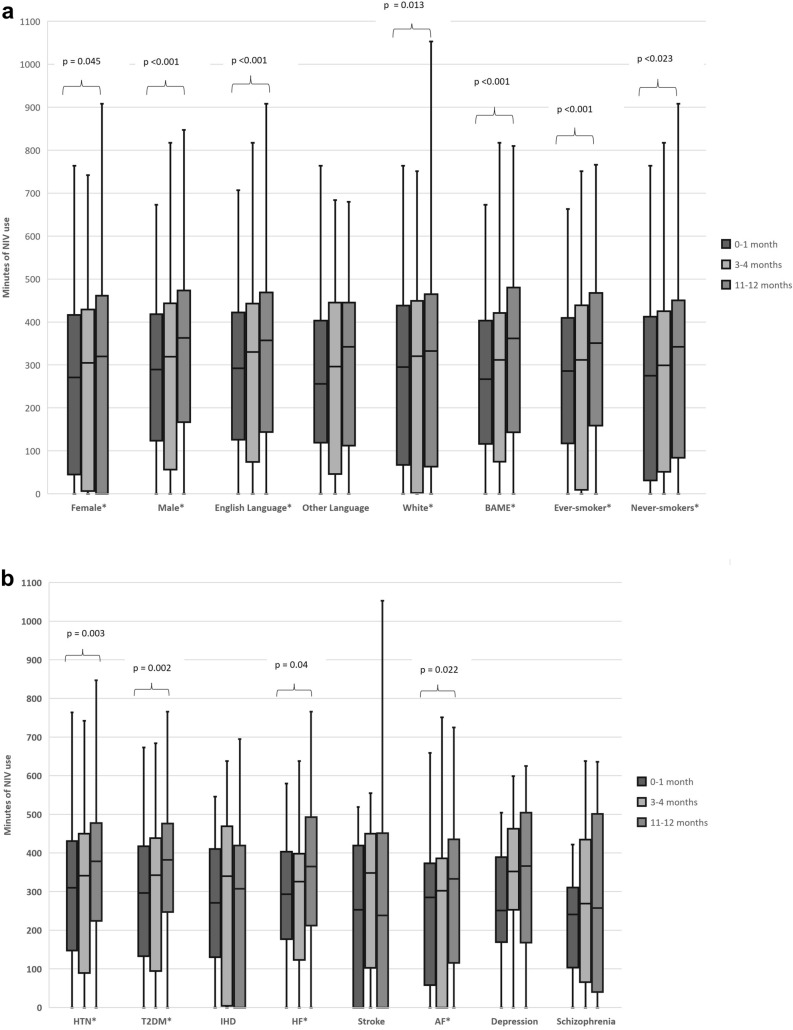
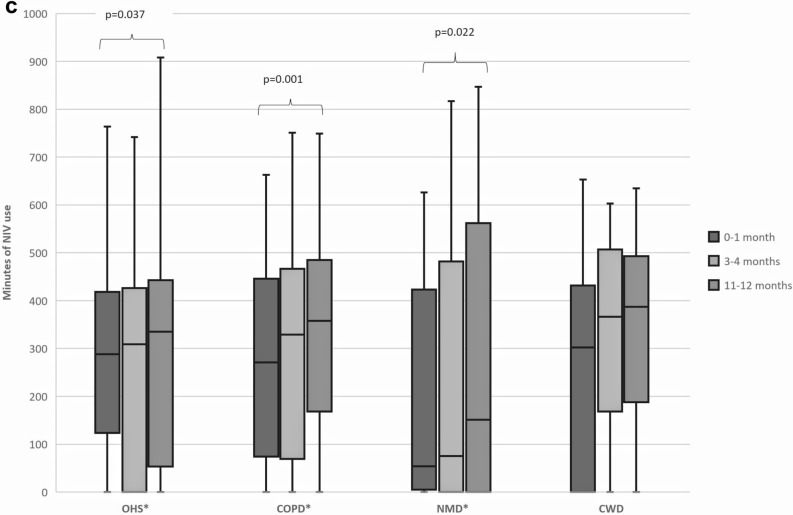
Few international studies have investigated factors affecting domiciliary non-invasive ventilation (D-NIV) compliance, and data from the UK are limited. We assessed compliance (defined as ≥ 4 h/night for at least 70% of the time) in a retrospective UK population study, at three time points (0-1 month, 3-4 months and 11-12 months), for all patients commenced on D-NIV over a 5-year period. A total of 359 patients were included. Non-compliant vs. compliant patients were significantly younger (median age 64 (IQR 52-72) vs. 67 (58-75) years, p = 0.032) and more likely to have schizophrenia, consistent at both 3-4 months (5% vs. 1%, p = 0.033) and 11-12 months (5% vs. 2%, p = 0.049). Repeated measures ANOVA demonstrated that the minutes [median (IQR)] of D-NIV used significantly increased at the three time points (0-1 month, 3-4 months and 11-12 months) for patients with hypertension [310 (147.5-431) vs. 341 (89-450) vs. 378 (224.5-477.5), p = 0.003]; diabetes [296.5 (132.5-417.5) vs. 342.5 (94.5-438.5) vs. 382 (247.5-476.25), p = 0.002] and heart failure [293 (177-403) vs. 326 (123-398) vs. 365 (212-493), p = 0.04]. In conclusion, younger and comorbid schizophrenic patients have lower D-NIV compliance rates, and our data suggest that persistence with D-NIV over a year may improve overall use.
Keywords: Compliance; Non-invasive ventilation; Schizophrenia.
© 2022. The Author(s).
Conflict of interest statement
All authors have completed the ICMJE-unified disclosure forms. AJS and AA have received support for attending conferences by Dolby Vivisol (not in relation to this work). SM has received educational sponsorship from Philips and Dolby Vivisol and grants from Philips (not in relation to this work). SwM has done consulting work for Philips and received educational sponsorship and support for attending conferences by Dolby Vivisol (not in relation to this work). The other authors have no conflicts of interest to declare.
Figures
References
-
- Köhnlein T, Windisch W, Köhler D, et al. Non-invasive positive pressure ventilation for the treatment of severe stable chronic obstructive pulmonary disease: a prospective, multicentre, randomised, controlled clinical trial. Lancet Respir Med. 2014;2:698–705. doi: 10.1016/S2213-2600(14)70153-5. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
