

Chronic active Epstein-Barr exacerbated by COVID-19 co-infection
- PMID: 35872097
- PMCID: PMC9303058
- DOI: 10.1016/j.ijid.2022.07.046
Chronic active Epstein-Barr exacerbated by COVID-19 co-infection
Abstract
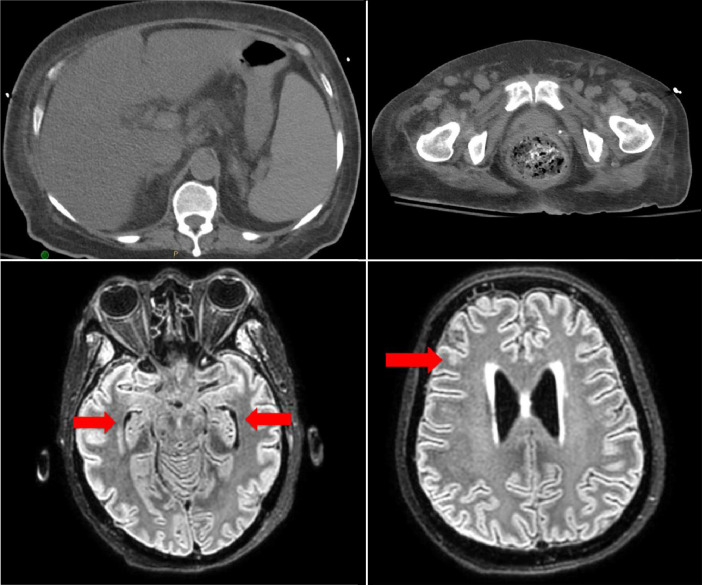
A 60-year-old Hispanic female was admitted with recurrent fevers, altered mental status, lymphadenopathy, hepatosplenomegaly, and pancytopenia. Initially, sepsis was presumed because of recurrent urinary tract infection with extended-spectrum beta-lactamase Escherichia coli. Despite appropriate therapy, her clinical condition continued to decline. An extensive workup was obtained to determine the source of her ailments. Bone marrow biopsy was negative for leukemia, lymphoma, and myelodysplastic syndrome; fluorescence in situ hybridization and a cytogenetic panel were normal; a lumbar puncture was negative. However, peripheral blood was remarkable for elevated titers for Epstein-Barr virus (EBV) consistent with chronic active EBV. Treatment with valganciclovir showed early positive results, but the patient became co-infected with COVID-19, and her EBV titer increased again, resulting in a precipitous health decline and death.
Keywords: COVID-19; Chronic active Epstein-Barr; Co-infection; Epstein-Barr virus; SARS-CoV-2.
Copyright © 2022 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors have no competing interests to declare.
Figures
References
-
- Cohen JI. Epstein-Barr virus infection. N Engl J Med. 2000;343:481–492. - PubMed
-
- Dunmire SK, Verghese PS, Balfour HH., Jr. Primary Epstein-Barr virus infection. J Clin Virol. 2018;102:84–92. - PubMed
-
- Ishida Y, Yokota Y, Tauchi H, et al. Ganciclovir for chronic active Epstein-Barr virus infection. Lancet. 1993;341:560–561. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
