

Association of left ventricular diastolic function with coronary artery calcium score: A Project Baseline Health Study
- PMID: 35872137
- PMCID: PMC10870833
- DOI: 10.1016/j.jcct.2022.06.003
Association of left ventricular diastolic function with coronary artery calcium score: A Project Baseline Health Study
Abstract
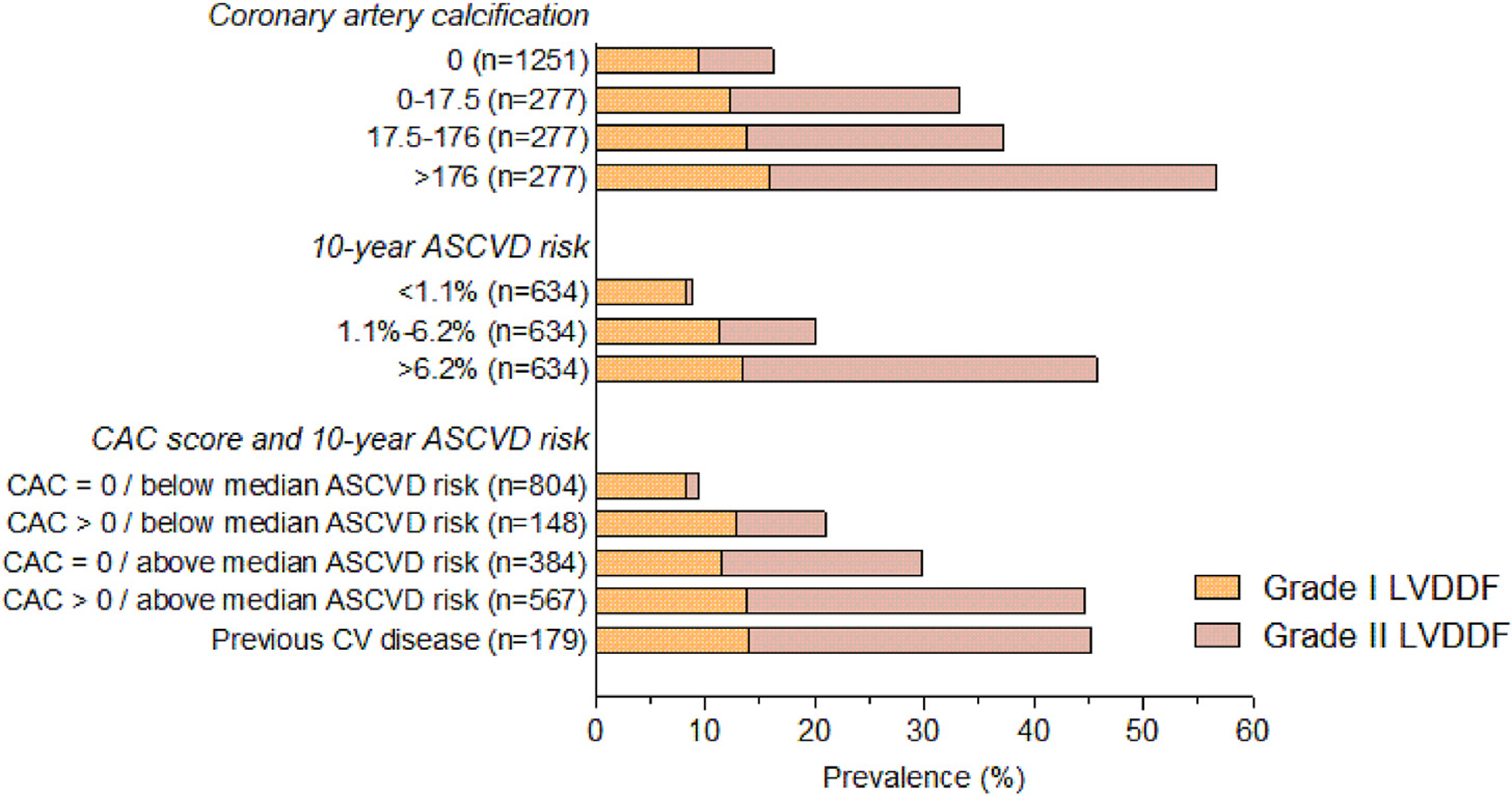
Background: Coronary artery calcium (CAC) and left ventricular diastolic dysfunction (LVDD) are strong predictors of cardiovascular events and share common risk factors. However, their independent association remains unclear.
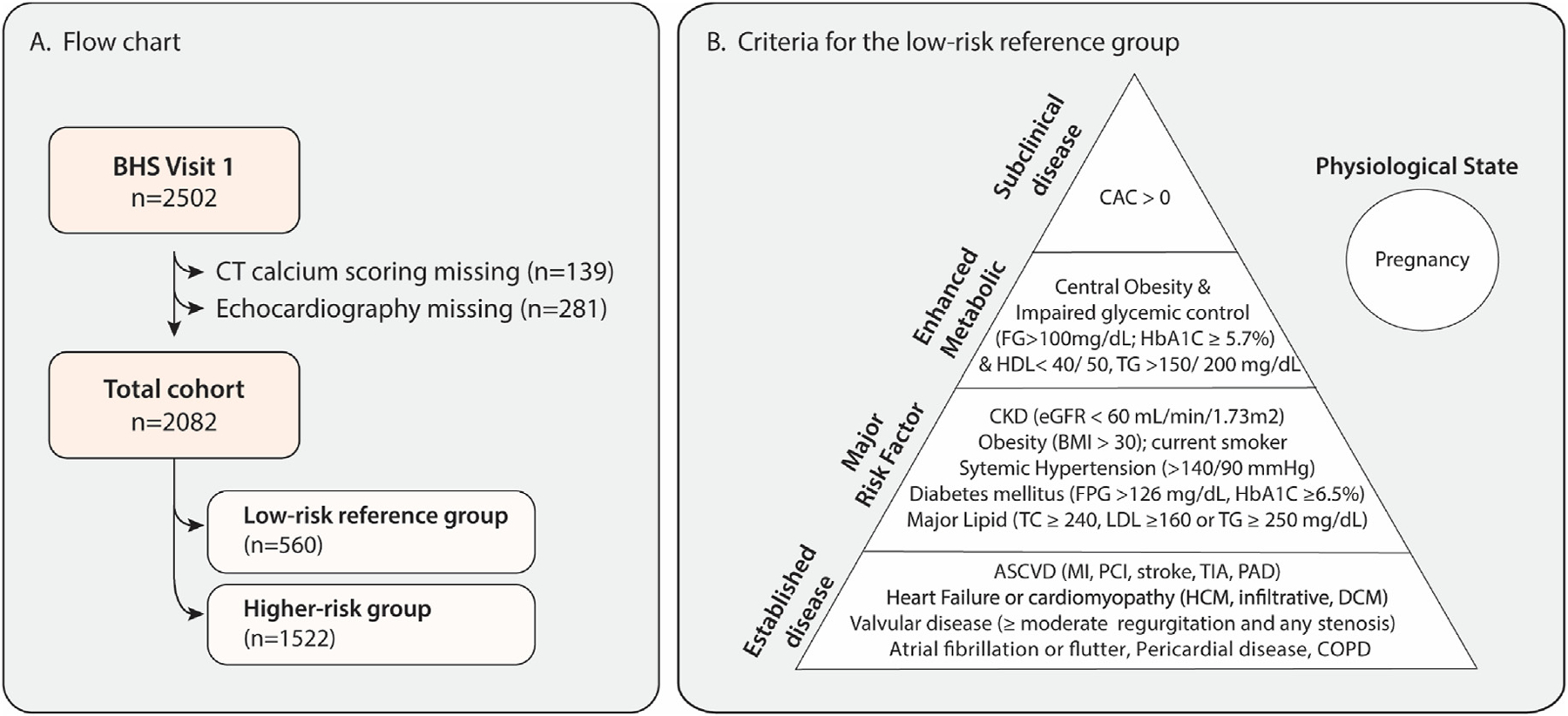
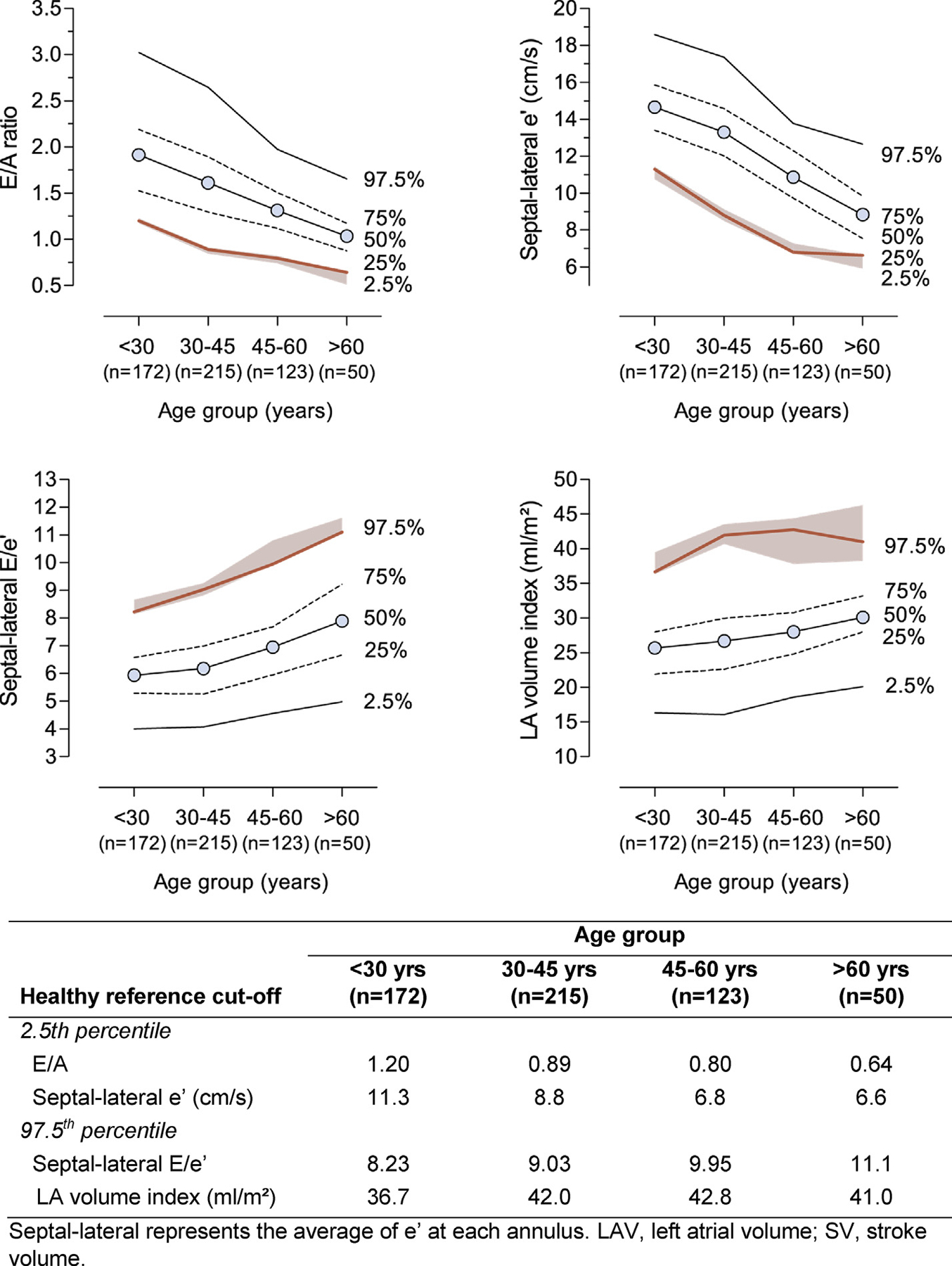
Methods: In the Project Baseline Health Study (PBHS), 2082 participants underwent cardiac-gated, non-contrast chest computed tomography (CT) and echocardiography. The association between left ventricular (LV) diastolic function and CAC was assessed using multidimensional network and multivariable-adjusted regression analyses. Multivariable analysis was conducted on continuous LV diastolic parameters and categorical classification of LVDD and adjusted for traditional cardiometabolic risk factors. LVDD was defined using reference limits from a low-risk reference group without established cardiovascular disease, cardiovascular risk factors or evidence of CAC, (n = 560). We also classified LVDD using the American Society of Echocardiography recommendations.
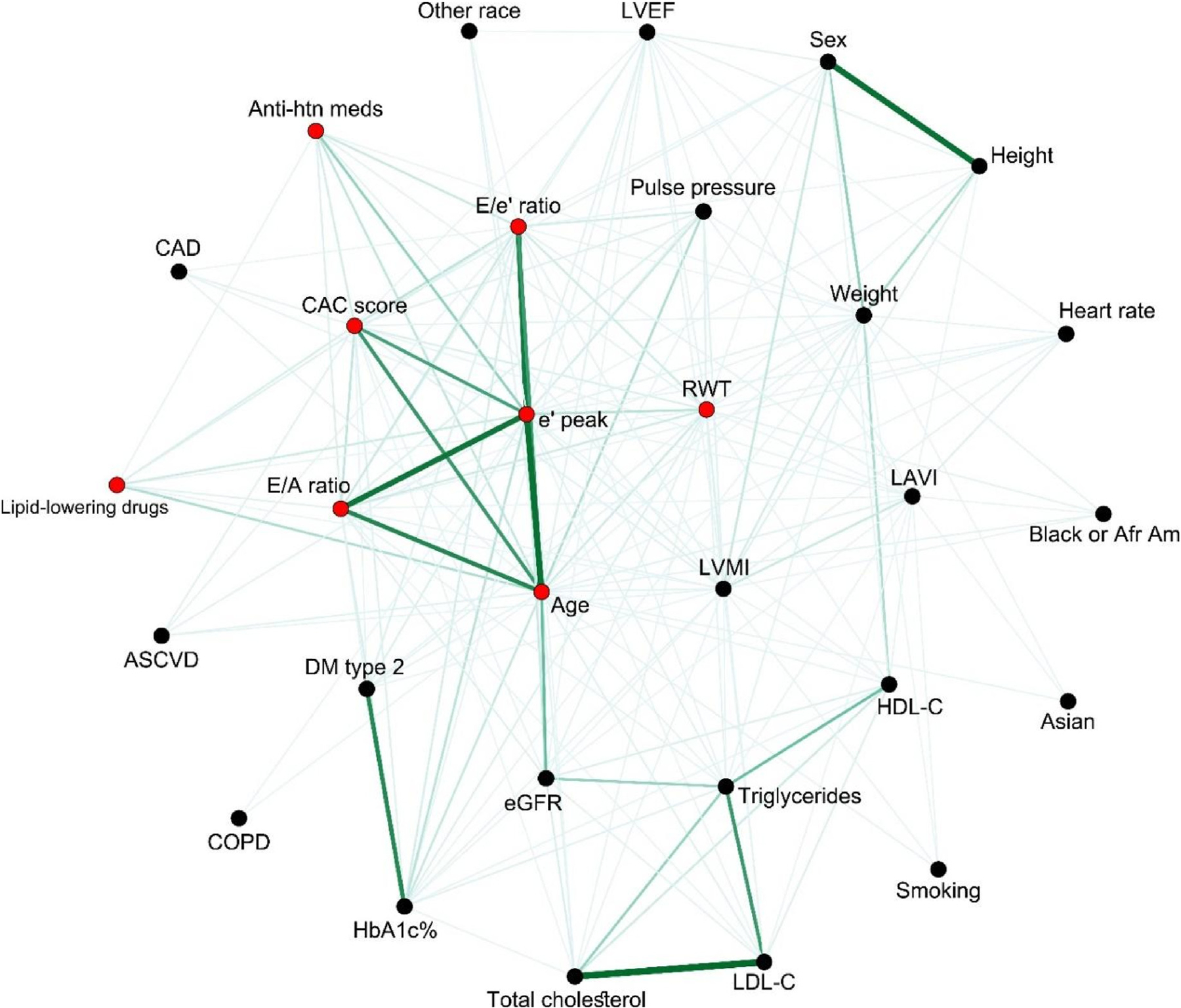
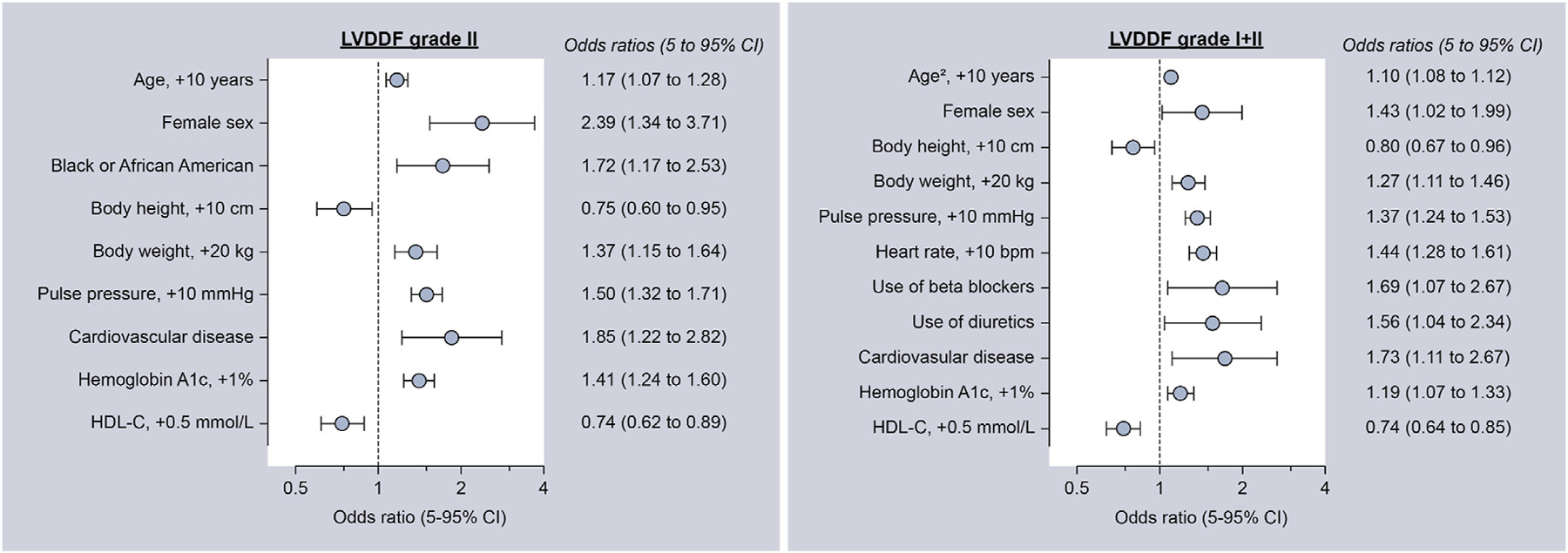
Results: The mean age of the participants was 51 ± 17 years with 56.6% female and 62.6% non-Hispanic White. Overall, 38.1% had hypertension; 13.7% had diabetes; and 39.9% had CAC >0. An intertwined network was observed between diastolic parameters, CAC score, age, LV mass index, and pulse pressure. In the multivariable-adjusted analysis, e', E/e', and LV mass index were independently associated with CAC after adjustment for traditional risk factors. For both e' and E/e', the effect size and statistical significance were higher across increasing CAC tertiles. Other independent correlates of e' and E/e' included age, female sex, Black race, height, weight, pulse pressure, hemoglobin A1C, and HDL cholesterol. The independent association with CAC was confirmed using categorical analysis of LVDD, which occurred in 554 participants (26.6%) using population-derived thresholds.
Conclusion: In the PBHS study, the subclinical coronary atherosclerotic disease burden detected using CAC scoring was independently associated with diastolic function.
Gov identifier: NCT03154346.
Keywords: Blood pressure; Cardiovascular disease; Coronary artery calcium; Coronary artery disease; Heart failure; Hypertension; Left ventricular diastolic dysfunction.
Copyright © 2022. Published by Elsevier Inc.
Conflict of interest statement
Declaration of competing interest All authors acknowledge institutional research grants from Verily Life Sciences. FH received an institutional research grant from Actelion Ltd. Within the last 2 years and an institutional research grant from Precordior Ltd. KM reports grants from Verily, Afferent, the American Heart Association (AHA), Cardiva Medical Inc, Gilead, Luitpold, Medtronic, Merck, Eidos, Ferring, Apple Inc, Sanifit, and St. Jude; grants and personal fees from Amgen, AstraZeneca, Bayer, CSL Behring, Johnson & Johnson, Novartis, and Sanofi; and personal fees from Anthos, Applied Therapeutics, Elsevier, Inova, Intermountain Health, Medscape, Mount Sinai, Mundi Pharma, Myokardia, Novo Nordisk, Otsuka, Portola, SmartMedics, and Theravance outside the submitted work. AH reports grants from Verily; grants and personal fees from AstraZeneca, Amgen, Bayer, Merck, and Novartis; and personal fees from Boston Scientific outside the submitted work. RC reports grants from Verily Life Sciences and Google Health, and personal fees from Cytokinetics Inc. And Centessa Inc. NC reports grants from the Research Foundation Flanders. FR reports equity from HealthPals and Carta, and advisory board and consulting fees from NovoNordisk, HealthPals, and Novartis. JB reports grants from the National Institutes of Health (U01-HL146382–03, R01-MD013493-03, D43TW009337, U01-HL123336–06, U01-HL142099-03, and D43 TW(01)1625-01) and royalties or licensing fees from UpToDate. The other authors have no conflicts of interest to disclose.
Figures
References
-
- Chetrit M, Cremer PC, Klein AL. Imaging of diastolic dysfunction in community-based epidemiological studies and randomized controlled trials of HFpEF. JACC Cardiovasc Imaging 2020;13:310–326. - PubMed
-
- Kuznetsova T, Herbots L, Lopez B, et al. Prevalence of left ventricular diastolic dysfunction in a general population. Circ Heart Fail 2009;2:105–112. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
