

American Indian/Alaska Native and black colon cancer patients have poorer cause-specific survival based on disease stage and anatomic site of diagnosis
- PMID: 35872382
- PMCID: PMC9482950
- DOI: 10.1016/j.canep.2022.102229
American Indian/Alaska Native and black colon cancer patients have poorer cause-specific survival based on disease stage and anatomic site of diagnosis
Abstract
Objectives: Studies of race-specific colon cancer (CC) survival differences between right- vs. left-sided CC typically focus on Black and White persons and often consider all CC stages as one group. To more completely examine potential racial and ethnic disparities in side- and stage-specific survival, we evaluated 5-year CC cause-specific survival probabilities for five racial/ethnic groups by anatomic site (right or left colon) and stage (local, regional, distant).
Methods: We obtained cause-specific survival probability estimates from National Cancer Institute's population-based Surveillance, Epidemiology, and End Results (SEER) for CC patients grouped by five racial/ethnic groups (Non-Hispanic American Indian/Alaska Native [AIAN], Non-Hispanic Asian/Pacific Islander [API], Hispanic, Non-Hispanic Black [NHB], and Non-Hispanic White [NHW]), anatomic site, stage, and other patient and SEER registry characteristics. We used meta-regression approaches to identify factors that explained differences in cause-specific survival.
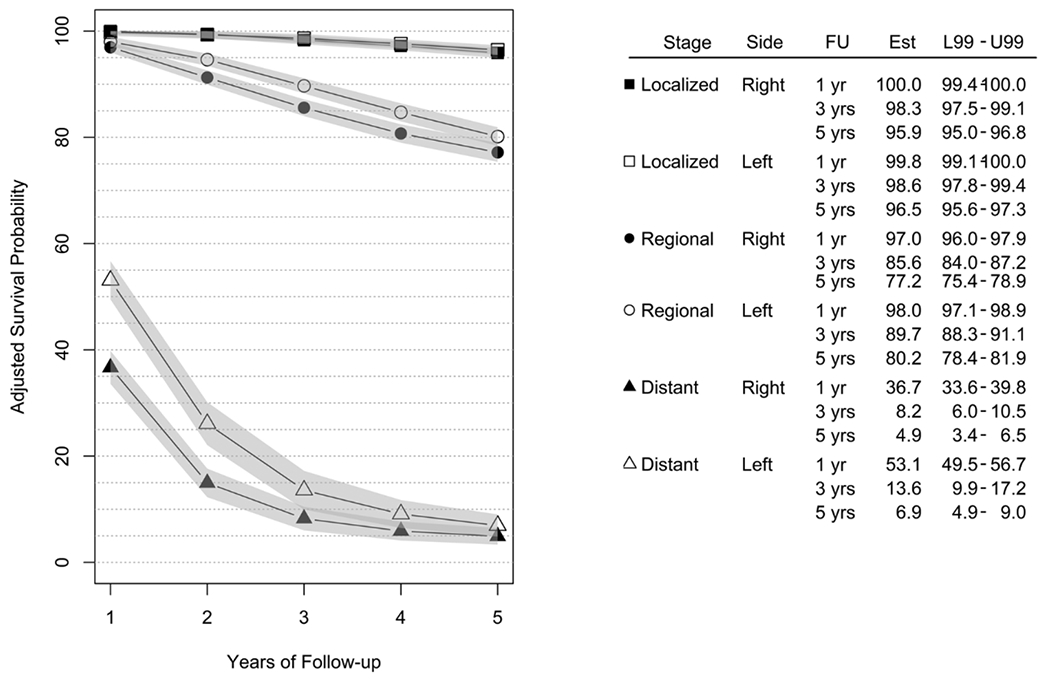
Results: Diagnoses of distant-stage CC were more common among NHB and AIAN persons (>22 %) than among NHW and API persons (< 20 %). Large disparities in anatomic site-specific survival were not apparent. Those with right-sided distant-stage CC had a one-year cause-specific survival probability that was 16.4 % points lower (99 % CI: 12.2-20.6) than those with left-sided distant-stage CC; this difference decreased over follow-up. Cause-specific survival probabilities were highest for API, and lowest for NHB, persons, though these differences varied substantially by stage at diagnosis. AIAN persons with localized-stage CC, and NHB persons with regional- and distant-stage CC, had significantly lower survival probabilities across follow-up.
Conclusions: There are differences in CC presentation according to anatomic site and disease stage among patients of distinct racial and ethnic backgrounds. This, coupled with the reality that there are persistent survival disparities, with NHB and AIAN persons experiencing worse prognosis, suggests that there are social or structural determinants of these disparities. Further research is needed to confirm whether these CC cause-specific survival disparities are due to differences in risk factors, screening patterns, cancer treatment, or surveillance, in order to overcome the existing differences in outcome.
Keywords: Colon cancer; Disparities; Minority health; Survival.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Conflict of Interest Statement All authors declare that they have no competing interests relating to the materials presented in the current manuscript.
Figures
References
-
- CDC Cancer, An Update on Cancer Deaths in the United States [Internet], Centers for Disease Control and Prevention, 2021. [cited 2021 Aug 14]. Available from: ⟨https://www.cdc.gov/cancer/dcpc/research/update-on-cancer-deaths/index.htm⟩.
-
- SEER Program, Cancer Stat Facts: Colorectal Cancer [Internet], National Cancer Institute, 2022. [cited 2022 Jul 1]. Available from: ⟨https://seer.cancer.gov/statfacts/html/colorect.html⟩.
-
- Howlander N, Noone AM, Krapcho M, Miller D, Brest A, Yu M, et al. , SEER Cancer Statistics Review, 1975–2018 [Internet], 2021. Available from: ⟨https://seer.cancer.gov/csr/1975_2018/⟩, based on November 2020 SEER data submission, posted to the SEER web site, April 2021.
-
- Siegel RL, Miller KD, Goding Sauer A, Fedewa SA, Butterly LF, Anderson JC, et al. Colorectal cancer statistics, 2020, CA Cancer J. Clin 70 (3) (2020) 145–164. - PubMed
-
- SEER Program, Cancer Stat Facts: Cancer Disparities [Internet], National Cancer Institute, 2022. [cited 2022 Jul 1]. Available from: ⟨https://seer.cancer.gov/statfacts/html/disparities.html⟩.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
