

Combined transcranial and transnasal endoscopic approach in transnasal-penetrating intracranial injury: A rare case report
- PMID: 35872549
- PMCID: PMC9403176
- DOI: 10.1016/j.ijscr.2022.107422
Combined transcranial and transnasal endoscopic approach in transnasal-penetrating intracranial injury: A rare case report
Abstract
Introduction: Transnasal-penetrating intracranial injuries are rare traumatic brain injuries that can cause serious and fatal brain damage and a high mortality rate and necessitate immediate multidisciplinary surgical management. We describe an uncommon case whereby a patient who presented with an accidental penetrating injury of the brain was found to have a wooden transnasal-penetrating intracranial object.
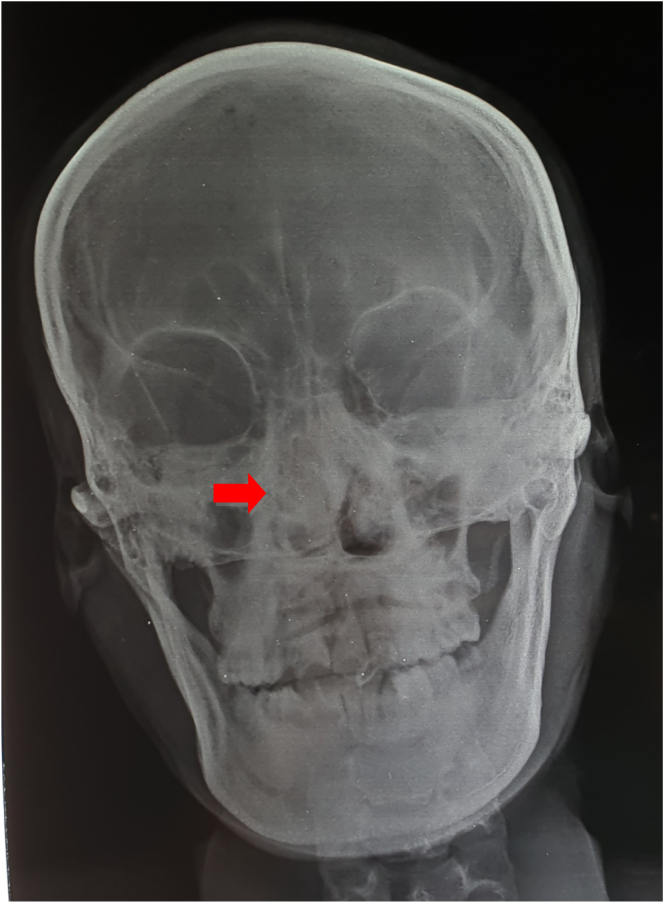
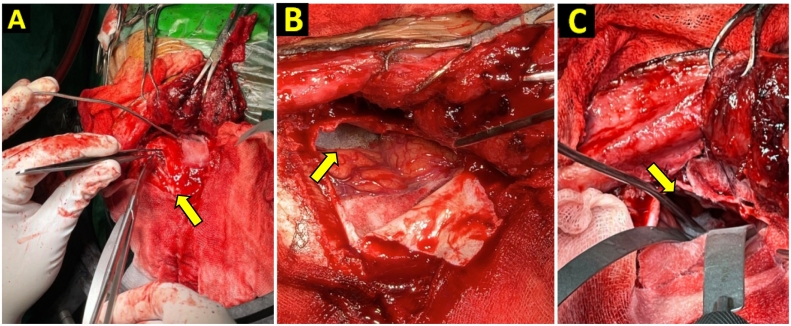
Case presentation: A 28-year-old man consulted an ear, nose, and throat (ENT) surgeon after complaints of headache for two days, a history of epistaxis, and vomitus. The right side of the nose had been punctured by wood as a result of falling from a motorcycle. A computed tomography (CT) scan led to diagnosis of a transnasal penetrating intracranial injury. Removal of the transcranial foreign body was carried out jointly by a neurosurgeon and ENT surgeon. Postoperatively, antibiotics were given for 14 days, and the patient was discharged without neurological deficit.
Clinical discussion: Early diagnostic procedures, such as CT scan of the skull to assess trajectory and extent of vascular and brain tissue injury, are required for appropriate surgical planning and post-operative treatment of such patients. Surgery was performed by combined transcranial and transnasal endoscopy to identify the skull base, dura mater defect, and brain tissue damage. Removal of the corpus alienum by transnasal endoscopy yielded a good outcome.
Conclusion: Combined transcranial and transnasal endoscopic approach showed better result than transcranial approach only. The wooden foreign body can be completely eliminated transnasally without active bleeding using this approach. The patient was discharged with good outcome.
Keywords: Case report; Endoscopic endonasal approach; Foreign body; Penetrating intracranial injury; Transcranial; Wooden object.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Nothing to declare.
Figures


References
-
- Asadullah A., Harmawan E.W., Prastikarunia R., Hutomo Putra G., Kustono H., Utama A.S., Artha K.S.A., Apriawan T., Bajamal A.H. Management of penetrating brain injury : a case report. Indones. J. Neurosurg. 2020;3:74–79. doi: 10.15562/ijn.v3i3.76. - DOI
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
