

Network Meta-Analysis of Perioperative Analgesic Effects of Different Interventions on Postoperative Pain After Arthroscopic Shoulder Surgery Based on Randomized Controlled Trials
- PMID: 35872801
- PMCID: PMC9304654
- DOI: 10.3389/fmed.2022.921016
Network Meta-Analysis of Perioperative Analgesic Effects of Different Interventions on Postoperative Pain After Arthroscopic Shoulder Surgery Based on Randomized Controlled Trials
Abstract
Background: Shoulder arthroscopic surgery is a common surgical method used in orthopedics. However, severe postoperative pain can significantly limit the early joint movement of patients and adversely affect the impact of the surgery. At present, there is no consistent and effective analgesic scheme for the management of postoperative pain after arthroscopic surgery of the shoulder.
Purpose: The aim of this study was to search for the most effective analgesic scheme to control pain in the perioperative period of arthroscopic surgery of the shoulder.
Study design: Network meta-analysis.
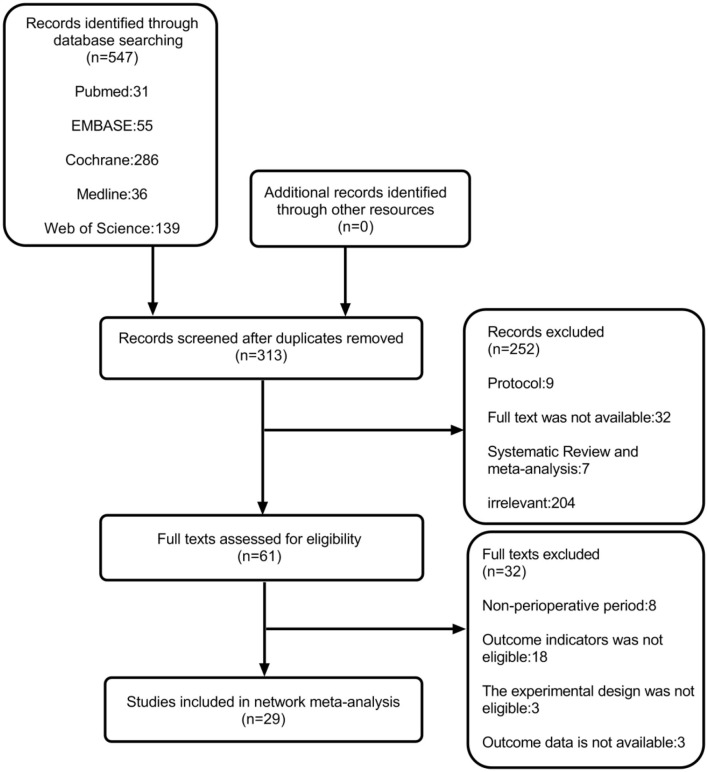
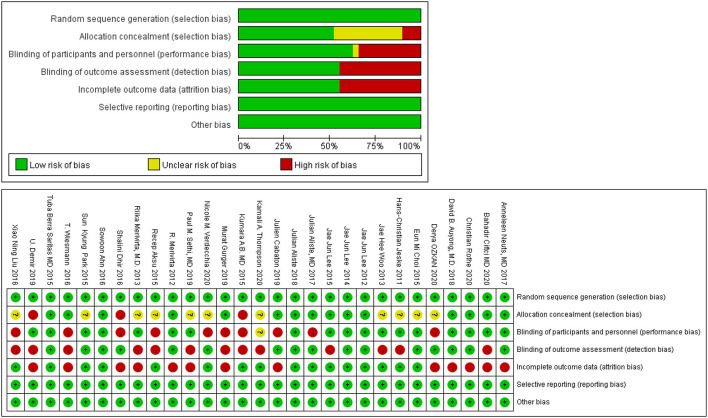
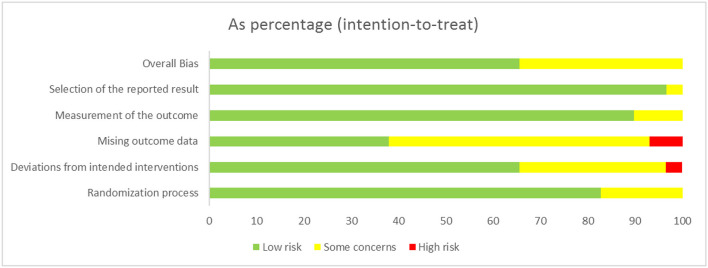
Methods: We searched 5 different databases (i.e., Medline, PubMed, Embase, Web of Science, and the Cochrane Library) from January 2011 to January 2021 for English literature. Thereafter, we sifted out randomized controlled trials (RCTs), which compared different intervention schemes for pain management after shoulder arthroscopy and selected only 12 h, 24 h, or 48 h after the patient leaves the operating room as an optimal period for administration of analgesic intervention schemes. Only patients with shoulder disease who have undergone arthroscopic shoulder surgery were included in this study. The Cochrane "risk of bias" was used for the quality assessment. Moreover, some additional tests were performed to enhance the credibility of the results.
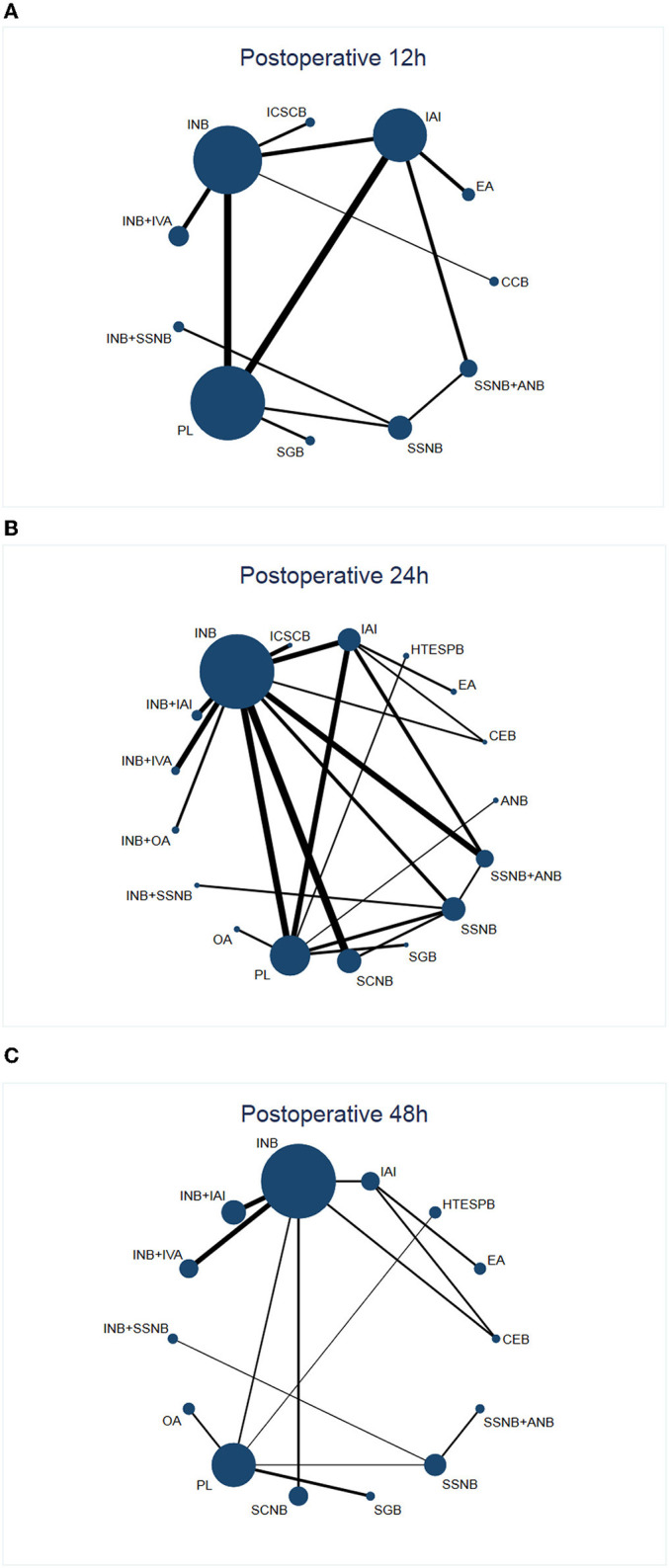
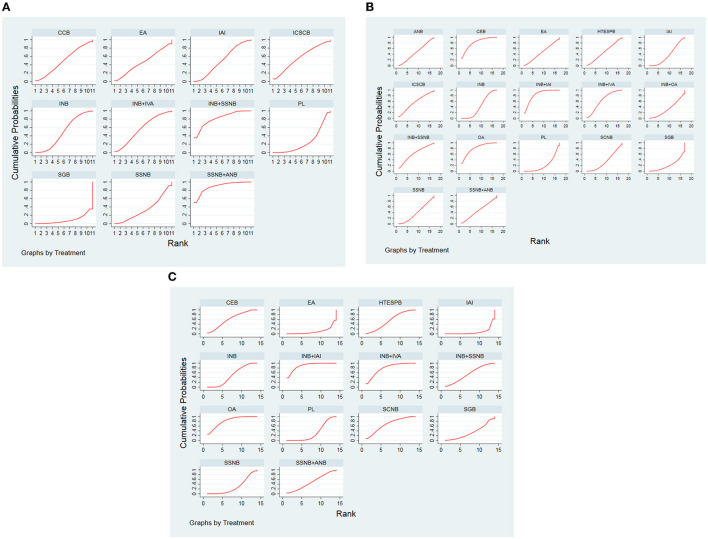
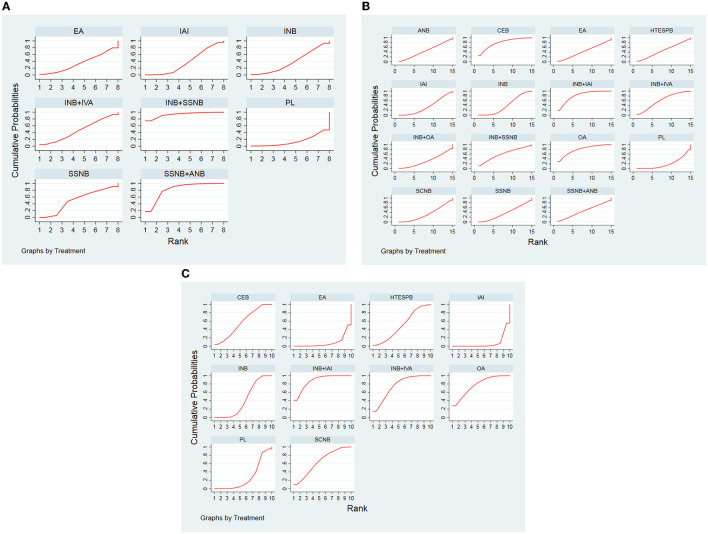
Results: Twenty-nine RCTs involving 1,885 patients were included in this frequentist network meta-analysis (NMA). These articles mainly were divided into two distinct groups, namely, the nerve block group and the non-nerve block group. Regarding the nerve block group, at postoperative 12 h, the intervention suprascapular nerve block + interscalene nerve block (SSNB + INB) was ranked first, whereas INB + intra-articular injection (INB + IAI) was ranked first at 24 h and 48 h postoperation. In the non-nerve block group, external application (EA) was ranked first at postoperative 12 h, but oral administration (OA) exhibited a better analgesic effect at postoperative 24 h and postoperative 48 h.
Conclusion: We conclude that the analgesic effect of SSNB+INB was the best at postoperative 12 h, and INB+IAI was the best at postoperative 24 h and 48 h in the nerve block group. For the non-nerve block group, the effect of EA was the best at postoperative 12 h, and the analgesic effect of OA at postoperative 24 h and 48 h was significantly better than any other interventions.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier: CRD42021286777.
Keywords: arthroscopic shoulder surgery; network meta-analysis; pair-wise meta-analysis; postoperative pain; randomized controlled trials.
Copyright © 2022 Jiangping, Xiaolin, Han, Zhou, Mao, Zhibo, Ting, Shidong, Xiangwei, Xin and Guoyin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources