

Pharmacokinetic/Pharmacodynamic Target Attainment of Vancomycin, at Three Reported Infusion Modes, for Methicillin-Resistant Staphylococcus aureus (MRSA) Bloodstream Infections in Critically Ill Patients: Focus on Novel Infusion Mode
- PMID: 35873144
- PMCID: PMC9300975
- DOI: 10.3389/fcimb.2022.874401
Pharmacokinetic/Pharmacodynamic Target Attainment of Vancomycin, at Three Reported Infusion Modes, for Methicillin-Resistant Staphylococcus aureus (MRSA) Bloodstream Infections in Critically Ill Patients: Focus on Novel Infusion Mode
Abstract
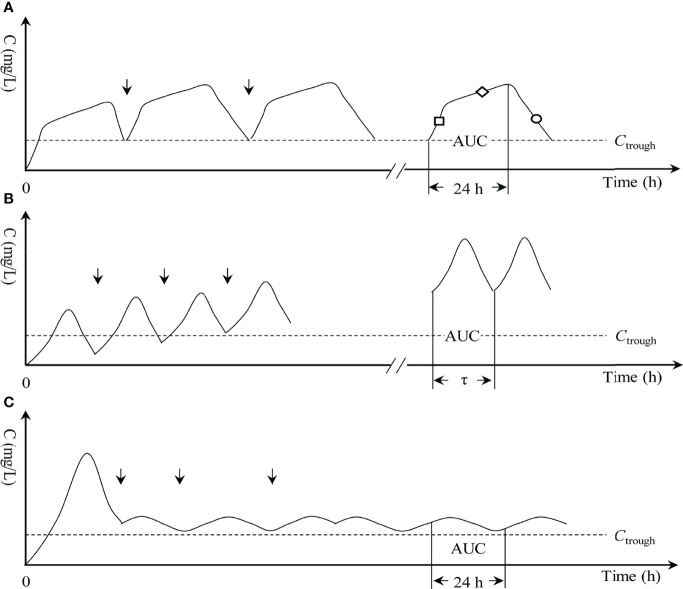
Objective: The study aimed to evaluate and compare the pharmacokinetic/pharmacodynamic (PK/PD) exposure to vancomycin in the novel optimal two-step infusion (OTSI) vs. intermittent infusion (II) vs. continuous infusion (CI) mode, for MRSA bloodstream infections occurring in critical patients.
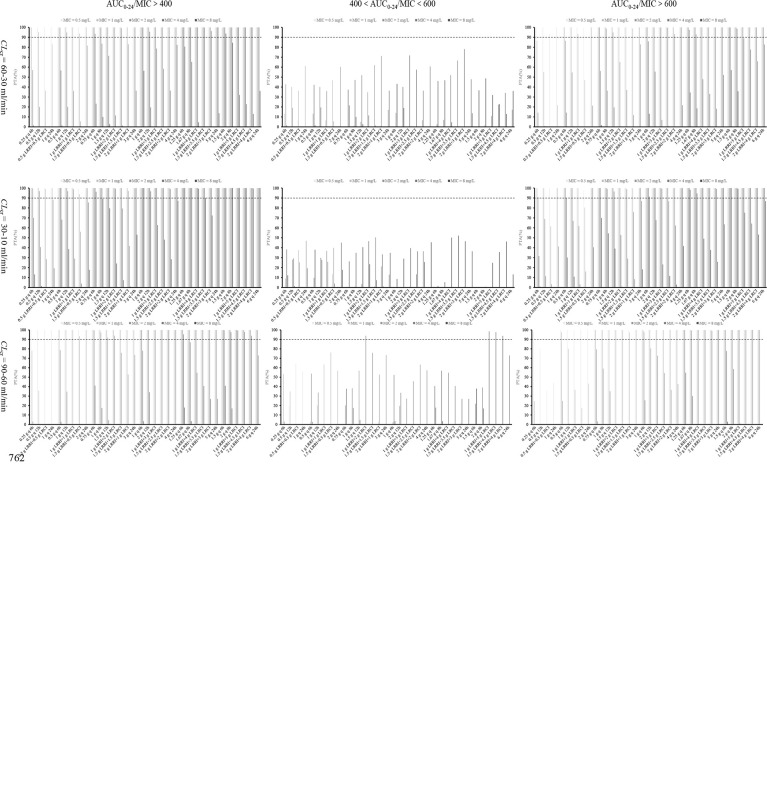
Methods: With PK/PD modeling and Monte Carlo simulations, the PK/PD exposure of 15 OTSI, 13 II, and 6 CI regimens for vancomycin, at 1, 2, 3, 4, 5, and 6 g daily dose, was evaluated. Using the Monte Carlo simulations, the vancomycin population PK parameters derived from critical patients, the PD parameter for MRSA isolates [i.e., minimum inhibitory concentration (MIC)], and the dosing parameters of these regimens were integrated into a robust mdel of vancomycin PK/PD index, defined as a ratio of the daily area under the curve (AUC0-24) to MIC (i.e., AUC0-24/MIC), to estimate the probability of target attainment (PTA) of these regimens against MRSA isolates with an MIC of 0.5, 1, 2, 4, and 8 mg/L in patients with varying renal function. The PTA at an AUC0-24/MIC ratio of >400, 400-600, and >600 was estimated. A regimen with a PTA of ≥90% at an AUC0-24/MIC ratio of 400-600, which is supposed to maximize both efficacy and safety, was considered optimal.
Results: At the same daily dose, almost only the OTSI regimens showed a PTA of ≥90% at an AUC0-24/MIC ratio of 400-600, and this profile seems evident especially in patients with creatinine clearance (CLcr) of ≥60 ml/min and for isolates with an MIC of ≤2 mg/L. However, for patients with CLcr of <60 ml/min and for isolates with an MIC of ≥4 mg/L, the II regimens often displayed a higher or even ≥90% PTA at an AUC0-24/MIC ratio of >400 and of >600. The CI regimens frequently afforded a reduced PTA at an AUC0-24/MIC ratio of >400 and of >600, regardless of CLcr and MIC.
Conclusions: The data indicated that the OTSI regimens allowed preferred PK/PD exposure in terms of both efficacy and safety, and thus should be focused more on, especially in patients with CLcr of ≥60 ml/min and for isolates with an MIC of ≤2 mg/L.
Keywords: continuous infusion; intermittent infusion; methicillin-resistant Staphylococcus aureus; optimal infusion; pharmacokinetic/pharmacodynamic; vancomycin.
Copyright © 2022 Song and Han.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Competence Mining of Vancomycin (VAN) in the Management of Infections Due to Bacterial Strains With High VAN Minimum Inhibitory Concentrations (MICs): A Novel Dosing Strategy Based on Pharmacokinetic/Pharmacodynamic Modeling.Front Microbiol. 2021 Apr 22;12:649757. doi: 10.3389/fmicb.2021.649757. eCollection 2021. Front Microbiol. 2021. PMID: 33967986 Free PMC article.
-
Evaluation of omadacycline regimens for community-acquired bacterial pneumonia patients infected with Staphylococcus Aureus by pharmacokinetic/pharmacodynamic analysis.J Chemother. 2024 Dec;36(8):709-716. doi: 10.1080/1120009X.2024.2343963. Epub 2024 Apr 22. J Chemother. 2024. PMID: 38650393
-
Pharmacodynamic comparison of different antimicrobial regimens against Staphylococcus aureus bloodstream infections with elevated vancomycin minimum inhibitory concentration.BMC Infect Dis. 2020 Jan 23;20(1):74. doi: 10.1186/s12879-020-4782-9. BMC Infect Dis. 2020. PMID: 31973753 Free PMC article.
-
Use of vancomycin pharmacokinetic-pharmacodynamic properties in the treatment of MRSA infections.Expert Rev Anti Infect Ther. 2010 Jan;8(1):95-106. doi: 10.1586/eri.09.123. Expert Rev Anti Infect Ther. 2010. PMID: 20014904 Free PMC article. Review.
-
Ceftobiprole: a review of a broad-spectrum and anti-MRSA cephalosporin.Am J Clin Dermatol. 2008;9(4):245-54. doi: 10.2165/00128071-200809040-00004. Am J Clin Dermatol. 2008. PMID: 18572975 Review.
Cited by
-
Data Mining Models in Prediction of Vancomycin-Intermediate Staphylococcus aureus in Methicillin-Resistant S. aureus (MRSA) Bacteremia Patients in a Clinical Care Setting.Microorganisms. 2025 Jan 7;13(1):101. doi: 10.3390/microorganisms13010101. Microorganisms. 2025. PMID: 39858869 Free PMC article.
-
Modeling of pharmacokinetic/pharmacodynamic parameters in regular intermittent intravenous infusion and translational application of the models in personalized antibiotics dosing.J Transl Med. 2025 Jul 19;23(1):806. doi: 10.1186/s12967-025-06832-5. J Transl Med. 2025. PMID: 40684203 Free PMC article.
References
-
- Akers K. S., Cota J. M., Chung K. K., Renz E. M., Mende K., Murray C. K. (2012). Serum Vancomycin Levels Resulting From Continuous or Intermittent Infusion in Critically Ill Burn Patients With or Without Continuous Renal Replacement Therapy. J. Burn. Care Res. 33, e254–e262. doi: 10.1097/BCR.0b013e31825042fa - DOI - PubMed
-
- Deryke C. A., Alexander D. P. (2009). Optimizing Vancomycin Dosing Through Pharmacodynamic Assessment Targeting Area Under the Concentration-Time Curve/Minimum Inhibitory Concentration. Hosp. Pharm. 44, 751–765. doi: 10.1310/hpj4409-751 - DOI
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical