

The Microbiological Etiology of Fracture-Related Infection
- PMID: 35873162
- PMCID: PMC9300981
- DOI: 10.3389/fcimb.2022.934485
The Microbiological Etiology of Fracture-Related Infection
Abstract
Purpose: Fracture-related infection (FRI) is an important complication related to orthopaedic trauma. Although the scientific interest with respect to the diagnosis and treatment of FRI is increasing, data on the microbiological epidemiology remains limited. Therefore, the primary aim of this study was to evaluate the microbiological epidemiology related to FRI, including the association with clinical symptoms and antimicrobial susceptibility data. The secondary aim was to analyze whether there was a relationship between the time to onset of infection and the microbiological etiology of FRI.
Methods: FRI patients treated at the University Hospitals of Leuven, Belgium, between January 1st 2015 and November 24th 2019 were evaluated retrospectively. The microbiological etiology and antimicrobial susceptibility data were analyzed. Patients were classified as having an early (<2 weeks after implantation), delayed (2-10 weeks) or late-onset (> 10 weeks) FRI.
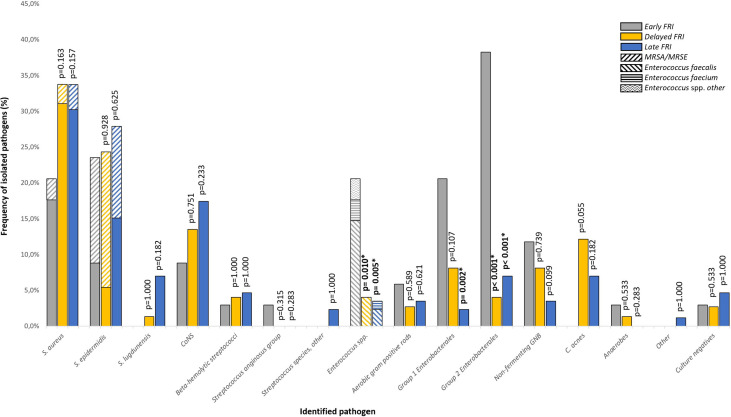
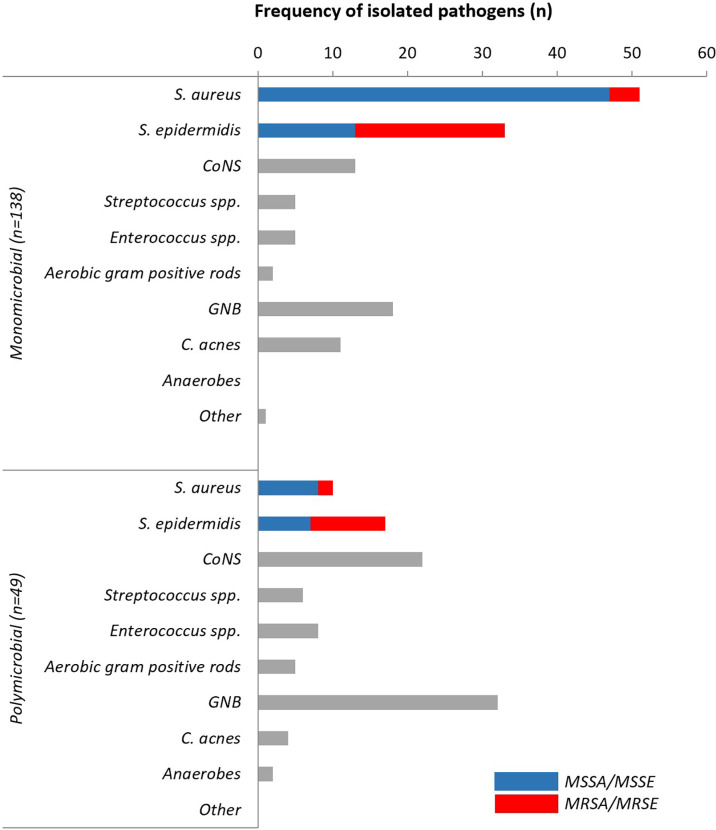
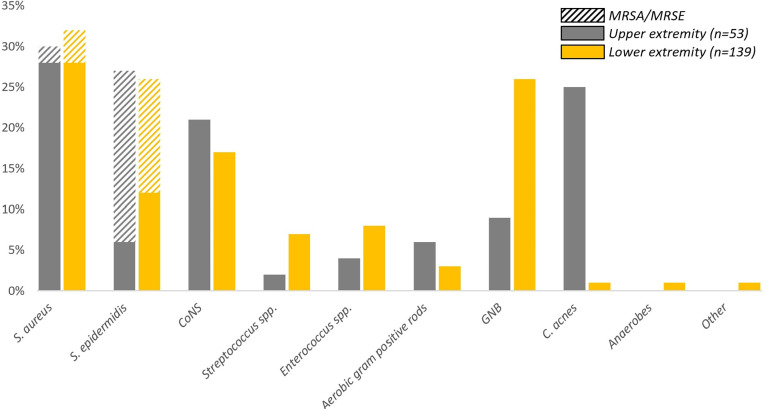
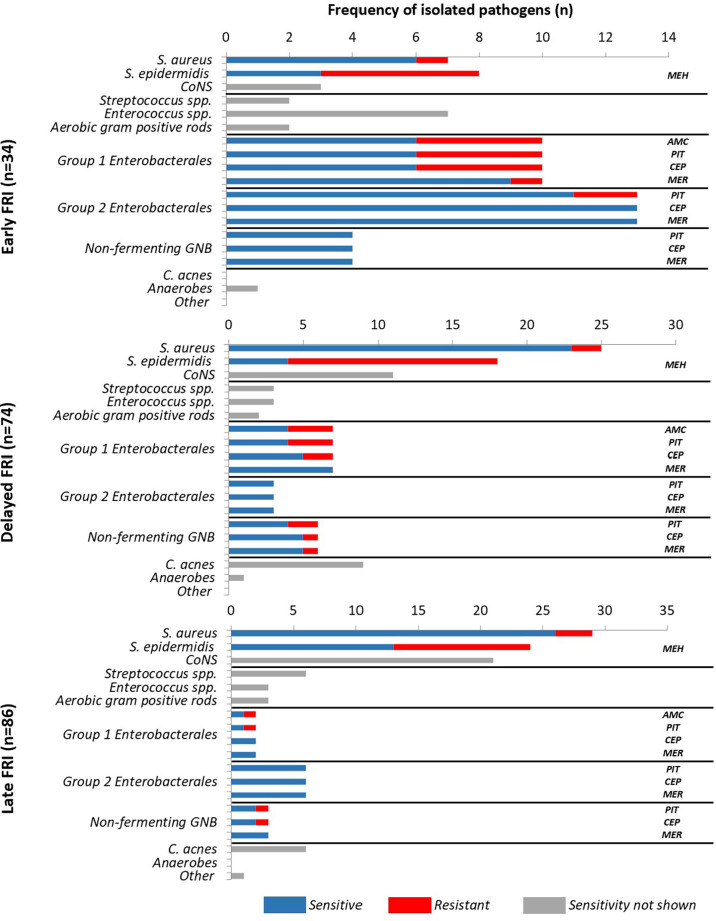
Results: One hundred ninety-one patients with 194 FRIs, most frequently involving the tibia (23.7%) and femur (18.6%), were included. Staphylococcus aureus was the most frequently isolated pathogen, regardless of time to onset (n=61; 31.4%), followed by S. epidermidis (n=50; 25.8%) and non-epidermidis coagulase-negative staphylococci (n=35; 18.0%). Polymicrobial infections (n=49; 25.3%), mainly involving Gram negative bacilli (GNB) (n=32; 65.3%), were less common than monomicrobial infections (n=138; 71.1%). Virulent pathogens in monomicrobial FRIs were more likely to cause pus or purulent discharge (n=45;54.9%; p=0.002) and fistulas (n=21;25.6%; p=0.030). Susceptibility to piperacillin/tazobactam for GNB was 75.9%. Vancomycin covered 100% of Gram positive cocci.
Conclusion: This study revealed that in early FRIs, polymicrobial infections and infections including Enterobacterales and enterococcal species were more frequent. A time-based FRI classification is not meaningful to estimate the microbiological epidemiology and cannot be used to guide empiric antibiotic therapy. Large multicenter prospective studies are necessary to gain more insight into the added value of (broad) empirical antibiotic therapy.
Keywords: antibiotic resistance; fracture; fracture-related infection; infection; microbiology.
Copyright © 2022 Depypere, Sliepen, Onsea, Debaveye, Govaert, IJpma, Zimmerli and Metsemakers.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Aboltins C. A., Dowsey M. M., Buising K. L., Peel T. N., Daffy J. R., Choong P. F., et al. (2011). Gram-Negative Prosthetic Joint Infection Treated With Debridement, Prosthesis Retention and Antibiotic Regimens Including a Fluoroquinolone. Clin. Microbiol. Infect. 17 (6), 862–867. doi: 10.1111/j.1469-0691.2010.03361.x - DOI - PubMed
-
- Baertl S., Walter N., Engelstaedter U., Ehrenschwender M., Hitzenbichler F., Alt V., et al. (2022). What Is the Most Effective Empirical Antibiotic Treatment for Early, Delayed, and Late Fracture-Related Infections? Antibiotics (Basel) 11 (3), 287. doi: 10.3390/antibiotics11030287 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources