

Infant Formula With a Specific Blend of Five Human Milk Oligosaccharides Drives the Gut Microbiota Development and Improves Gut Maturation Markers: A Randomized Controlled Trial
- PMID: 35873420
- PMCID: PMC9298649
- DOI: 10.3389/fnut.2022.920362
Infant Formula With a Specific Blend of Five Human Milk Oligosaccharides Drives the Gut Microbiota Development and Improves Gut Maturation Markers: A Randomized Controlled Trial
Abstract
Background: Human milk oligosaccharides (HMOs) have important biological functions for a healthy development in early life.
Objective: This study aimed to investigate gut maturation effects of an infant formula containing five HMOs (2'-fucosyllactose, 2',3-di-fucosyllactose, lacto-N-tetraose, 3'-sialyllactose, and 6'-sialyllactose).
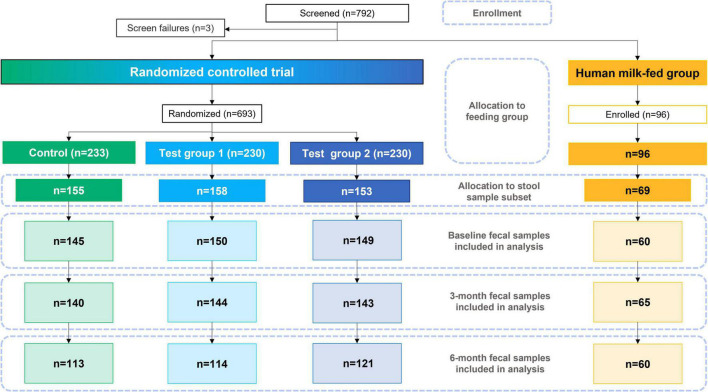
Methods: In a multicenter study, healthy infants (7-21 days old) were randomly assigned to a standard cow's milk-based infant formula (control group, CG); the same formula with 1.5 g/L HMOs (test group 1, TG1); or with 2.5 g/L HMOs (test group 2, TG2). A human milk-fed group (HMG) was enrolled as a reference. Fecal samples collected at baseline (n∼150/formula group; HMG n = 60), age 3 (n∼140/formula group; HMG n = 65) and 6 (n∼115/formula group; HMG n = 60) months were analyzed for microbiome (shotgun metagenomics), metabolism, and biomarkers.
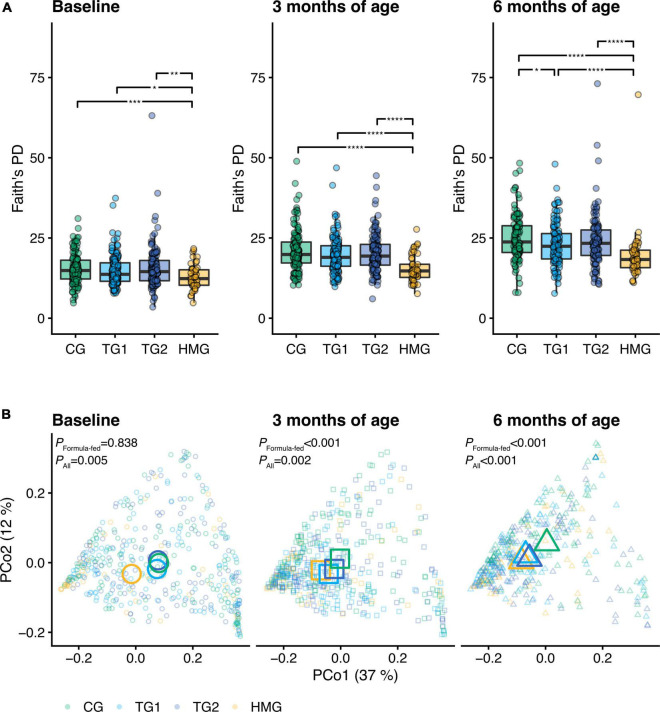
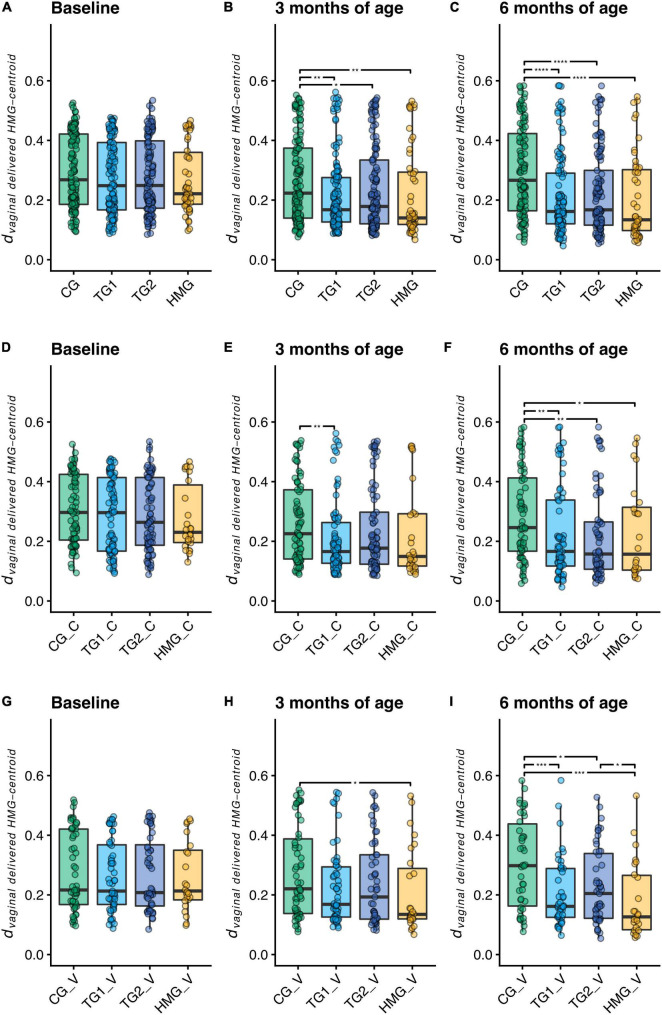
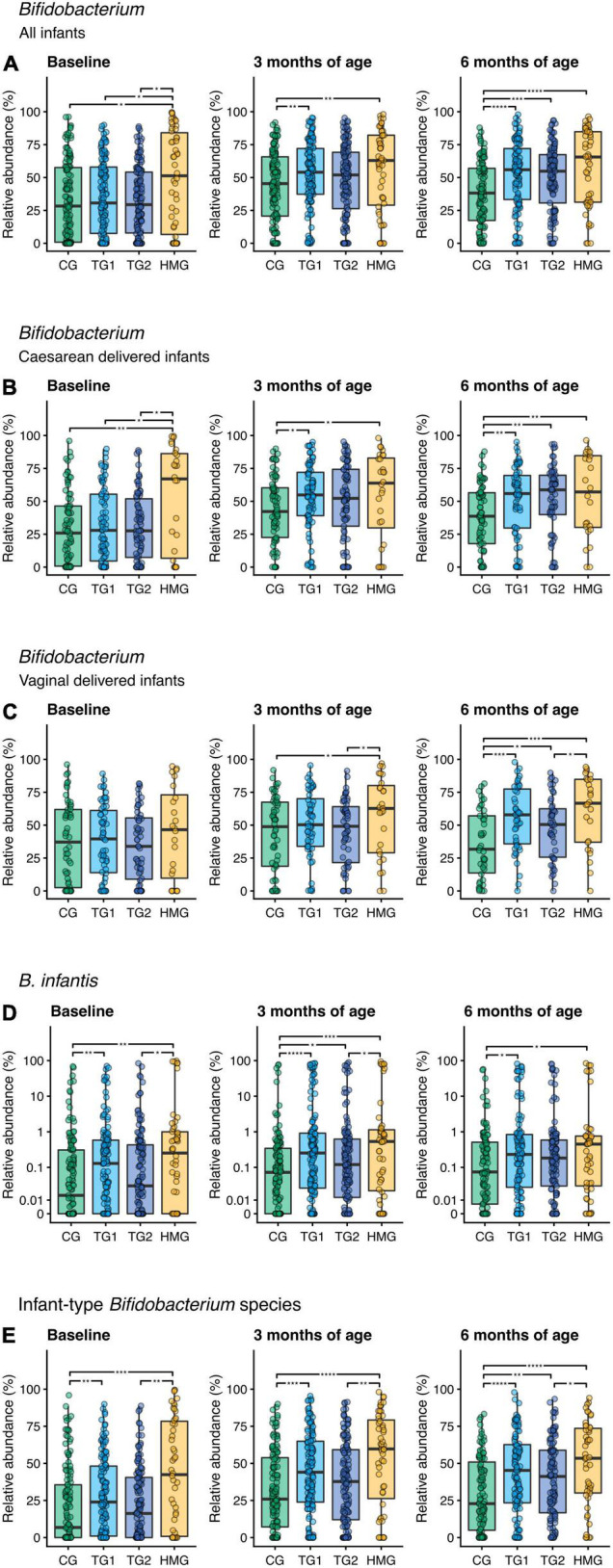
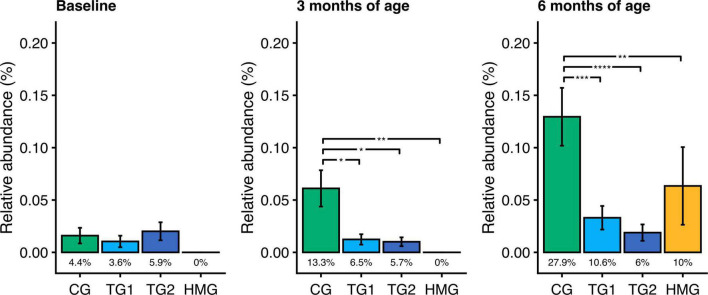
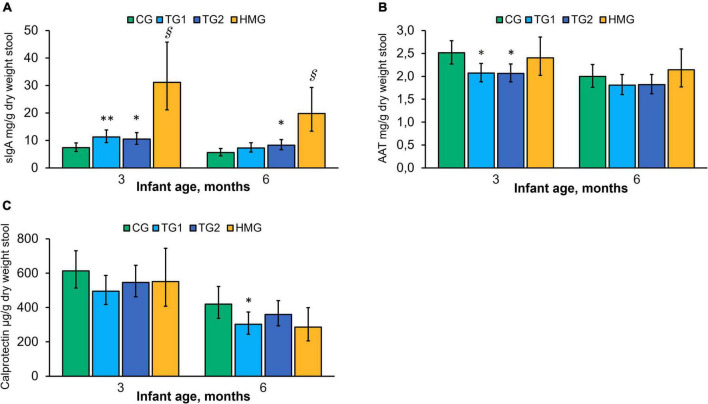
Results: At both post-baseline visits, weighted UniFrac analysis indicated different microbiota compositions in the two test groups (TGs) compared to CG (P < 0.01) with coordinates closer to that of HMG. The relative abundance of Bifidobacterium longum subsp. infantis (B. infantis) was higher in TGs vs. CG (P < 0.05; except at 6 months: TG2 vs. CG P = 0.083). Bifidobacterium abundance was higher by ∼45% in TGs vs. CG at 6-month approaching HMG. At both post-baseline visits, toxigenic Clostridioides difficile abundance was 75-85% lower in TGs vs. CG (P < 0.05) and comparable with HMG. Fecal pH was significantly lower in TGs vs. CG, and the overall organic acid profile was different in TGs vs. CG, approaching HMG. At 3 months, TGs (vs. CG) had higher secretory immunoglobulin A (sIgA) and lower alpha-1-antitrypsin (P < 0.05). At 6 months, sIgA in TG2 vs. CG remained higher (P < 0.05), and calprotectin was lower in TG1 (P < 0.05) vs. CG.
Conclusion: Infant formula with a specific blend of five HMOs supports the development of the intestinal immune system and gut barrier function and shifts the gut microbiome closer to that of breastfed infants with higher bifidobacteria, particularly B. infantis, and lower toxigenic Clostridioides difficile.
Clinical trial registration: [https://clinicaltrials.gov/ct2/show/], identifier [NCT03722550].
Keywords: Bifidobacterium longum subsp. infantis (B. infantis); Clostridioides (C.) difficile; bifidobacteria; gut maturation; gut microbiota; human milk oligosaccharides (HMOs); infant formula; intestinal immune response.
Copyright © 2022 Bosheva, Tokodi, Krasnow, Pedersen, Lukjancenko, Eklund, Grathwohl, Sprenger, Berger, Cercamondi and 5 HMO Study Investigator Consortium.
Conflict of interest statement
This study received funding from Nestlé Nutrition, Société des Produits Nestlé S.A., Switzerland. DG, NS, BB, and CC were current employees of the funder. The funder had the following involvement with the study: study design, data analysis, decision to publish, and preparation of the manuscript. HP, OL, and AE were employees of Clinical Microbiomics, Denmark, which was involved in the sample and data analysis. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Hamosh M. Bioactive factors in human milk. Pediatr Clin North Am. (2001) 48:69–86. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical