

BCI-FES With Multimodal Feedback for Motor Recovery Poststroke
- PMID: 35874158
- PMCID: PMC9296822
- DOI: 10.3389/fnhum.2022.725715
BCI-FES With Multimodal Feedback for Motor Recovery Poststroke
Abstract
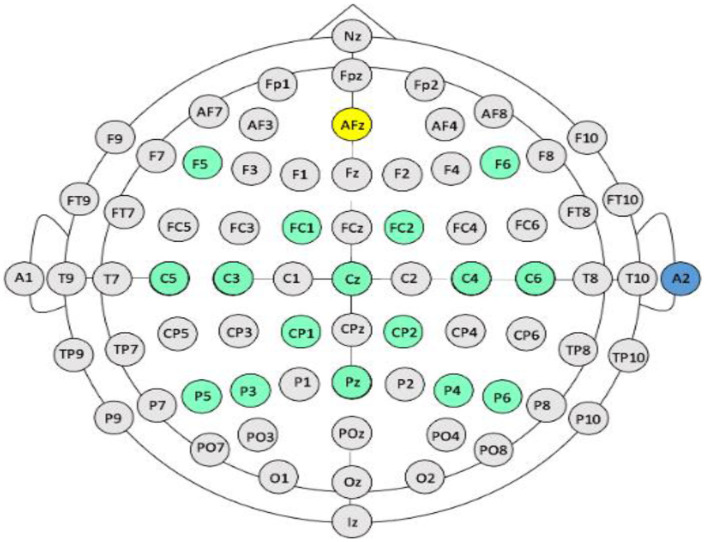
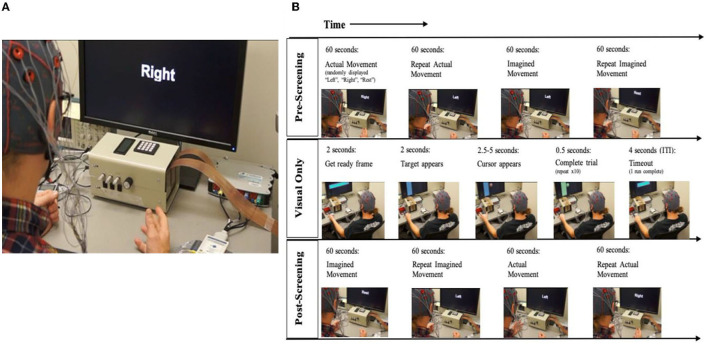
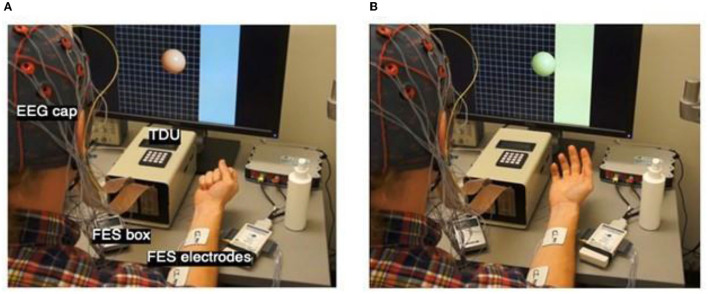
An increasing number of research teams are investigating the efficacy of brain-computer interface (BCI)-mediated interventions for promoting motor recovery following stroke. A growing body of evidence suggests that of the various BCI designs, most effective are those that deliver functional electrical stimulation (FES) of upper extremity (UE) muscles contingent on movement intent. More specifically, BCI-FES interventions utilize algorithms that isolate motor signals-user-generated intent-to-move neural activity recorded from cerebral cortical motor areas-to drive electrical stimulation of individual muscles or muscle synergies. BCI-FES interventions aim to recover sensorimotor function of an impaired extremity by facilitating and/or inducing long-term motor learning-related neuroplastic changes in appropriate control circuitry. We developed a non-invasive, electroencephalogram (EEG)-based BCI-FES system that delivers closed-loop neural activity-triggered electrical stimulation of targeted distal muscles while providing the user with multimodal sensory feedback. This BCI-FES system consists of three components: (1) EEG acquisition and signal processing to extract real-time volitional and task-dependent neural command signals from cerebral cortical motor areas, (2) FES of muscles of the impaired hand contingent on the motor cortical neural command signals, and (3) multimodal sensory feedback associated with performance of the behavioral task, including visual information, linked activation of somatosensory afferents through intact sensorimotor circuits, and electro-tactile stimulation of the tongue. In this report, we describe device parameters and intervention protocols of our BCI-FES system which, combined with standard physical rehabilitation approaches, has proven efficacious in treating UE motor impairment in stroke survivors, regardless of level of impairment and chronicity.
Keywords: brain-computer interface; closed-loop system; functional electrical stimulation; motor functional recovery; motor recovery; neurorehabilitation; open-loop system; stroke.
Copyright © 2022 Remsik, van Kan, Gloe, Gjini, Williams, Nair, Caldera, Williams and Prabhakaran.
Conflict of interest statement
JW is a scientific board member and has stock interests in NeuroOne Medical Inc., a company developing next generation epilepsy monitoring devices. JW also has an equity interest in NeuroNexus technology Inc., a company that supplies electrophysiology equipment and multichannel probes to the neuroscience research community. JW also has an equity interest in Neuraworx Medical Technologies Inc., a company developing non-invasive neuromodulation devices for treating cognitive impairments. None of these associations are directly relevant to the work presented in this manuscript. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Annetta N. V., Friend J., Schimmoeller A., Buck V. S., Friedenberg D. A., Bouton C. E., et al. (2019). A high definition noninvasive neuromuscular electrical stimulation system for cortical control of combinatorial rotary hand movements in a human with tetraplegia. IEEE Trans. Biomed. Eng. 66, 910–919. 10.1109/TBME.2018.2864104 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous