

Impact of Machine Perfusion on the Immune Response After Liver Transplantation - A Primary Treatment or Just a Delivery Tool
- PMID: 35874758
- PMCID: PMC9304705
- DOI: 10.3389/fimmu.2022.855263
Impact of Machine Perfusion on the Immune Response After Liver Transplantation - A Primary Treatment or Just a Delivery Tool
Abstract
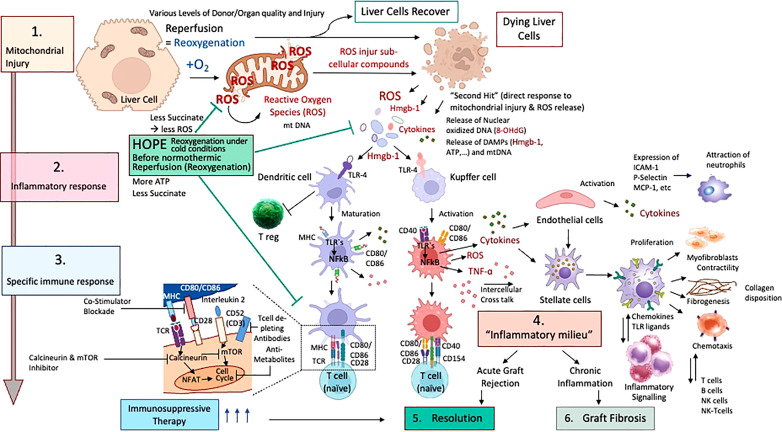
The frequent use of marginal livers forces transplant centres to explore novel technologies to improve organ quality and outcomes after implantation. Organ perfusion techniques are therefore frequently discussed with an ever-increasing number of experimental and clinical studies. Two main approaches, hypothermic and normothermic perfusion, are the leading strategies to be introduced in clinical practice in many western countries today. Despite this success, the number of studies, which provide robust data on the underlying mechanisms of protection conveyed through this technology remains scarce, particularly in context of different stages of ischemia-reperfusion-injury (IRI). Prior to a successful clinical implementation of machine perfusion, the concept of IRI and potential key molecules, which should be addressed to reduce IRI-associated inflammation, requires a better exploration. During ischemia, Krebs cycle metabolites, including succinate play a crucial role with their direct impact on the production of reactive oxygen species (ROS) at mitochondrial complex I upon reperfusion. Such features are even more pronounced under normothermic conditions and lead to even higher levels of downstream inflammation. The direct consequence appears with an activation of the innate immune system. The number of articles, which focus on the impact of machine perfusion with and without the use of specific perfusate additives to modulate the inflammatory cascade after transplantation is very small. This review describes first, the subcellular processes found in mitochondria, which instigate the IRI cascade together with proinflammatory downstream effects and their link to the innate immune system. Next, the impact of currently established machine perfusion strategies is described with a focus on protective mechanisms known for the different perfusion approaches. Finally, the role of such dynamic preservation techniques to deliver specific agents, which appear currently of interest to modulate this posttransplant inflammation, is discussed together with future aspects in this field.
Keywords: hypothermic oxygenated perfusion; innate immune activation; ischemia reperfusion injury; machine perfusion; marginal livers; mitochondrial injury.
Copyright © 2022 Panconesi, Flores Carvalho, Dondossola, Muiesan, Dutkowski and Schlegel.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- Colaneri J. An Overview of Transplant Immunosuppression–History, Principles, and Current Practices in Kidney Transplantation. Nephrol Nurs J (2014) 41:549–60; quiz 561. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical