

Demographics and Characteristics of Patients Admitted With Acute Coronary Syndrome to the Coronary Care Unit at King Abdulaziz University
- PMID: 35875268
- PMCID: PMC9298687
- DOI: 10.7759/cureus.26113
Demographics and Characteristics of Patients Admitted With Acute Coronary Syndrome to the Coronary Care Unit at King Abdulaziz University
Abstract
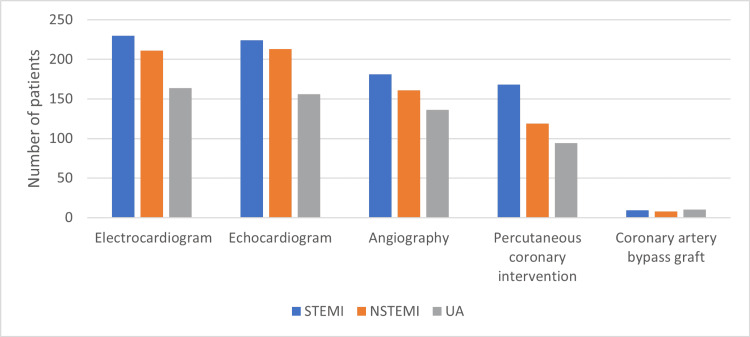
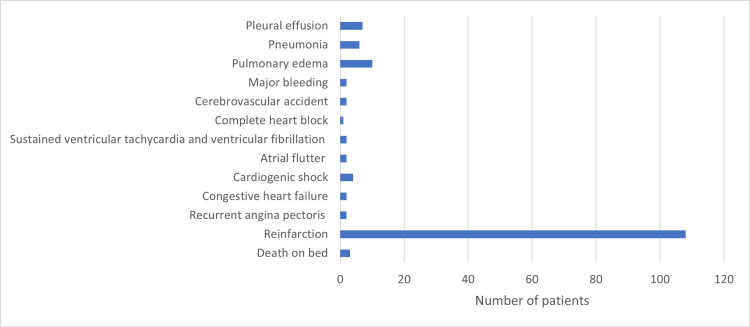
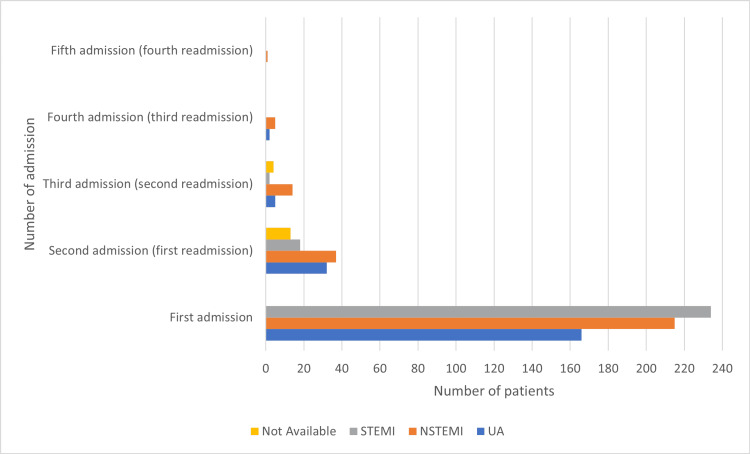
Background Over the previous decade, the incidence of cardiovascular diseases (CVDs) has risen in the Middle East and will increase mortality to 23 million individuals in Saudi Arabia by 2030, according to the Saudi Ministry of Health. CVDs, including acute coronary syndrome (ACS), are the most common cause of mortality globally. This study aimed to analyze the demographic and clinical characteristics of patients with ACS admitted to the coronary care unit (CCU) in a tertiary hospital in Jeddah, Saudi Arabia. To the best of our knowledge, a lack of research in this region has been undertaken. Methods This retrospective records review study was conducted in a tertiary center in Jeddah, Saudi Arabia. All patients admitted to our CCU in 2017 with a final diagnosis of ACS were retrospectively enrolled. Demographic details, coronary risk factors, investigation and procedures, management, and clinical outcomes are all part of the data. Results Of the 615 patients included in the study, 491 (79.84%) were males, 226 (36.75%) were 55-64 years old, and 161 (26.18%) were 45-54 years old. Males had a higher rate of ST-segment elevation myocardial infarction (STEMI) (214, 43.58%), while females had a higher rate of non-ST-segment elevation myocardial infarction (NSTEMI) and unstable angina (UA) (45.96% and 37.90%, respectively). Diabetes (62.60%), dyslipidemia (62.44%), and hypertension (61.46%) were the most prevalent risk factors. Angiography and percutaneous coronary intervention (PCI) were performed in 77.72% and 61.95% of patients, respectively. Coronary artery bypass graft was only performed in 4.39% of patients. PCI was performed more frequently in patients with STEMI than in those with NSTEMI/UA (P < 0.001). A large majority of patients (99.5%) recovered and were discharged. Of the 161 (26.18%) patients who attended a follow-up visit, only 45 (33.08%) met the therapeutic objective of 1.8 mmol/L (70 mg/dl) of low-density lipoprotein cholesterol. There were 100 (16.26%) patients readmitted to the CCU, and most of these were readmitted within a year after initial admission. Readmissions were more common in females and patients diagnosed with NSTEMI/UA during initial admission (15.47% and 19.35%, respectively). Conclusion This study revealed that our most common demographics were males between 45 and 64 years, which is a decade younger than the global average. STEMI was the most common presentation. The most common modifiable cardiovascular risk factors were hypertension, diabetes, and dyslipidemia. The most common adverse event was reinfarction, which was closely linked to hypertension and diabetes. In this study, the recovery rate was higher than in studies from other countries; however, the majority of patients did not achieve the goal of cholesterol levels at follow-up. Our population's younger age at presentation necessitates greater attention and more stringent preventive strategies, such as lifestyle changes and evidence-based treatments for CVD risk factors, to reduce the incidence and burden of ACS on CCUs.
Keywords: acute coronary syndrome; cardiovascular diseases; coronary care unit; myocardial infarction; non-st elevation myocardial infraction; percutaneous coronary intervention; retrospective studies; saudi arabia; st-elevation myocardial infarction (stemi); unstable angina.
Copyright © 2022, Takieddin et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Current patterns of antithrombotic and revascularisation therapy in patients hospitalised for acute coronary syndromes. Data from the Polish subset of the EPICOR study.Kardiol Pol. 2017;75(5):445-452. doi: 10.5603/KP.a2017.0034. Epub 2017 Mar 10. Kardiol Pol. 2017. PMID: 28281731
-
Frequency of ST-segment elevation myocardial infarction, non-ST-segment myocardial infarction, and unstable angina: results from a Southwest Chinese Registry.Rev Cardiovasc Med. 2021 Mar 30;22(1):239-245. doi: 10.31083/j.rcm.2021.01.103. Rev Cardiovasc Med. 2021. PMID: 33792268
-
Epidemiology and risk factors of patients with types of acute coronary syndrome presenting to a tertiary care hospital in Sri Lanka.BMC Cardiovasc Disord. 2019 Oct 21;19(1):229. doi: 10.1186/s12872-019-1217-x. BMC Cardiovasc Disord. 2019. PMID: 31638908 Free PMC article.
-
Cardiovascular Risk Profile, Presentation and Management Outcomes of Patients with Acute Coronary Syndromes after Coronary Artery Bypass Grafting.Curr Probl Cardiol. 2022 Nov;47(11):101078. doi: 10.1016/j.cpcardiol.2021.101078. Epub 2021 Dec 11. Curr Probl Cardiol. 2022. PMID: 34902394 Review.
-
Contemporary NSTEMI management: the role of the hospitalist.Hosp Pract (1995). 2020 Feb;48(1):1-11. doi: 10.1080/21548331.2020.1701329. Epub 2020 Feb 20. Hosp Pract (1995). 2020. PMID: 31815570 Review.
Cited by
-
A Prospective Cross-Sectional Study of Acute Coronary Syndrome Patients' Quality of Life and Drug Prescription Patterns at Riyadh Region Hospitals, Saudi Arabia.Healthcare (Basel). 2023 Jul 7;11(13):1973. doi: 10.3390/healthcare11131973. Healthcare (Basel). 2023. PMID: 37444807 Free PMC article.
-
Support network: the challenges of ensuring myocardial infarction patients comfort in the critical care unit: a qualitative study.BMC Health Serv Res. 2024 Sep 12;24(1):1057. doi: 10.1186/s12913-024-11450-w. BMC Health Serv Res. 2024. PMID: 39267086 Free PMC article.
-
Risk Factors Associated With Coronary Disease in Saudi Arabia: A Comprehensive Review.Cureus. 2025 Feb 16;17(2):e79123. doi: 10.7759/cureus.79123. eCollection 2025 Feb. Cureus. 2025. PMID: 40109781 Free PMC article. Review.
References
-
- World Health Organization. Cardiovascular diseases. [ May; 2022 ];https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1 2021
-
- Acute coronary syndrome. Overbaugh KJ. Am J Nurs. 2009;109:42–52. - PubMed
-
- Chest pain, dyspnea and other symptoms in patients with type 1 and 2 myocardial infarction. A literature review. Lippi G, Sanchis-Gomar F, Cervellin G. Int J Cardiol. 2016;215:20–22. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous