

Recognizing Histopathological Simulators of Melanoma to Avoid Misdiagnosis
- PMID: 35875272
- PMCID: PMC9299949
- DOI: 10.7759/cureus.26127
Recognizing Histopathological Simulators of Melanoma to Avoid Misdiagnosis
Abstract
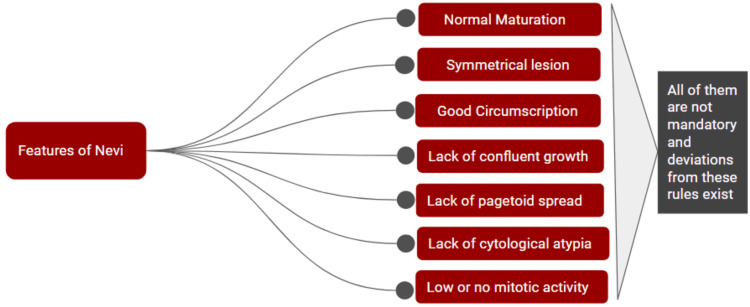
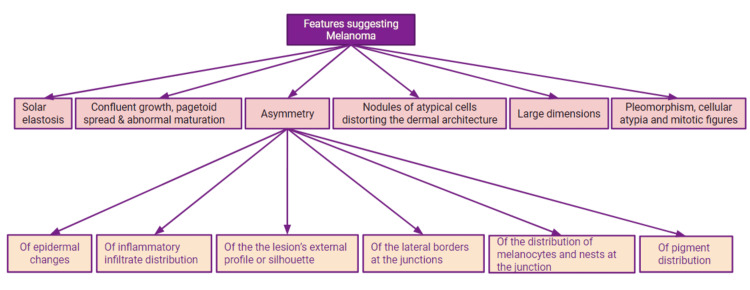
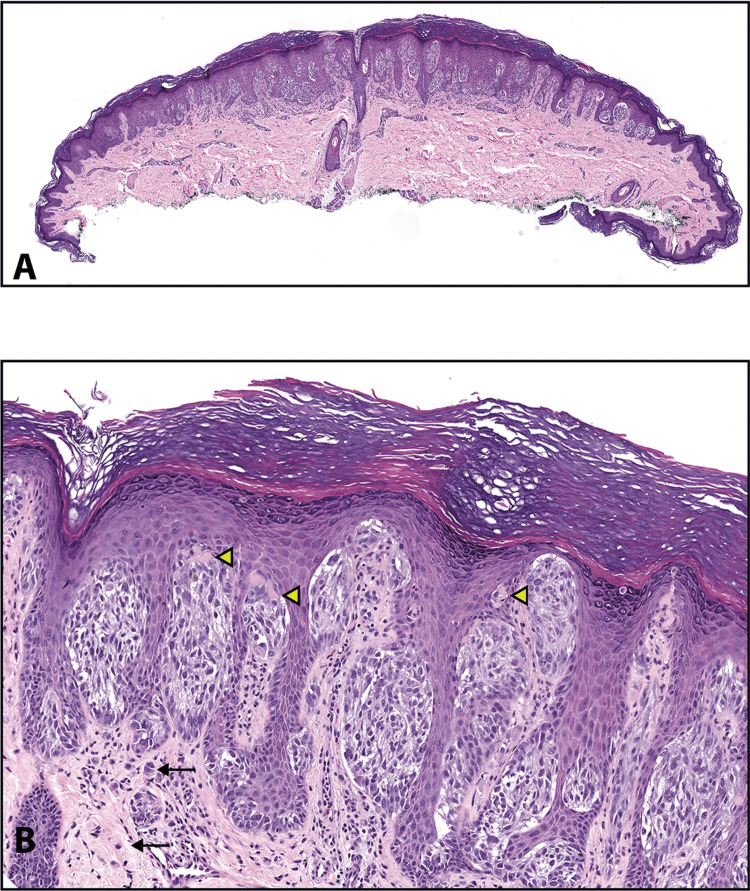
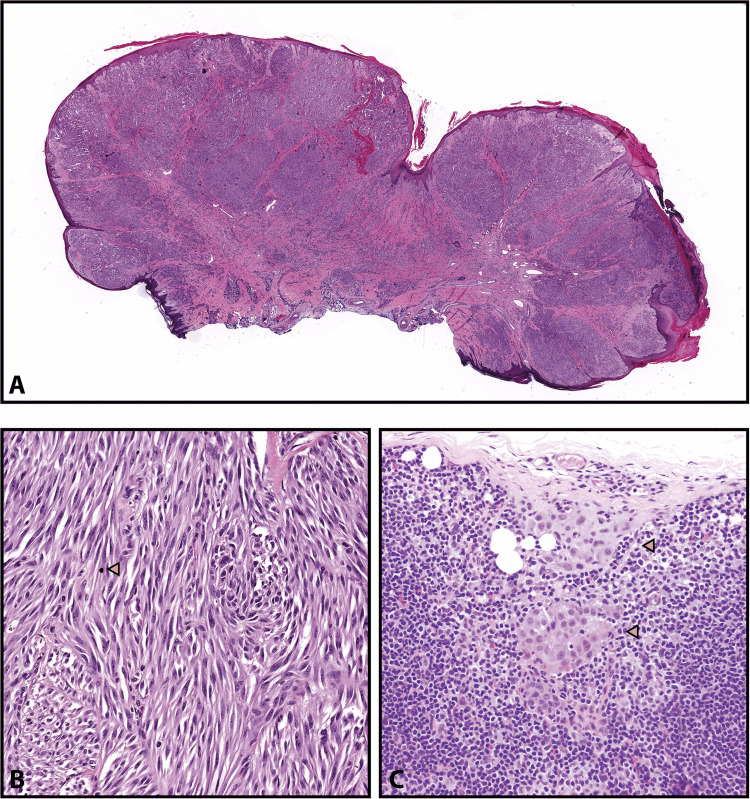
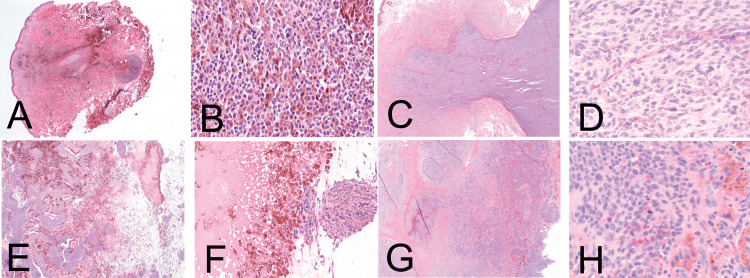
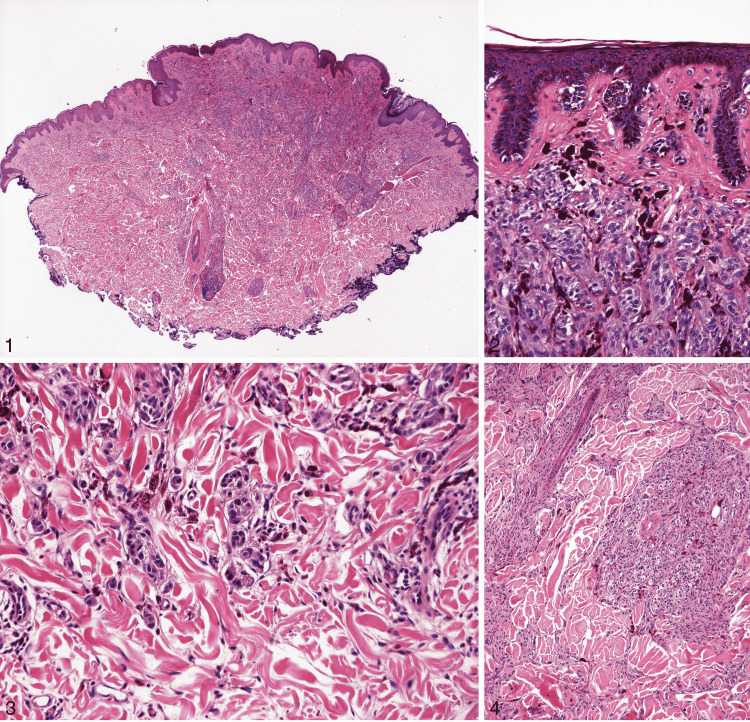
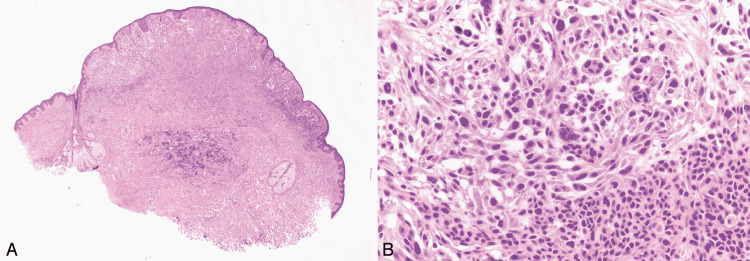
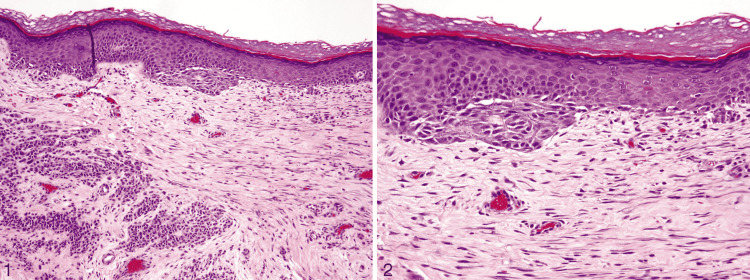
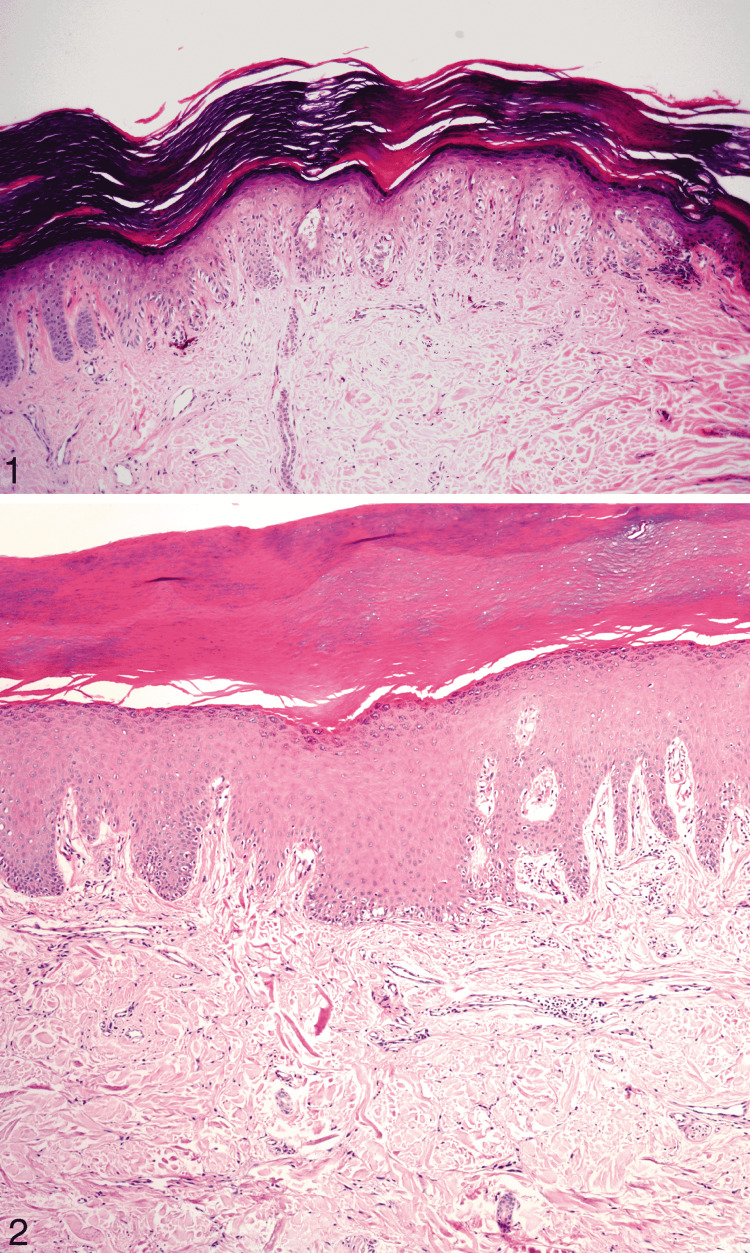
Melanocytic lesions have a wide morphological spectrum, ranging from benign nevi to malignant melanoma. In contrast to a diagnosis of a benign nevus, a diagnosis of melanoma could mean intensive treatment, lifetime monitoring, and a worse prognosis. Therefore, melanocytic tumors are notoriously challenging and associated with a high risk of litigation in surgical pathology. After describing the basic features of nevi and melanoma, this article describes the detailed clinical and histological features of those lesions that share many similar features with melanoma. The entities included are Spitz nevi and atypical Spitz tumors (AST), Reed nevus, dysplastic nevus, cellular blue nevus (CBN), deep penetrating nevus, combined nevus, recurrent nevus, irritated nevus, congenital pattern nevus, acral nevus, and nevi of special sites. Knowledge of these imitators can help pathologists distinguish between benign and malignant cases and avoid misdiagnosis.
Keywords: acral nevus; cellular blue nevus; congenital nevus; deep penetrating nevus; dysplastic nevus; melanocytic nevus; recurrent nevus; reed nevus; spitz tumors; melanoma and nevi.
Copyright © 2022, Waqar et al.
Conflict of interest statement
This article has copyrighted material in the form of histopathological images, used with permission from © 2019 Innovative Pathology Press and Archives of Pathology & Laboratory Medicine, © 2010 College of American Pathologists.
Figures



Similar articles
-
A Comparative Demographic Study of Atypical Spitz Nevi and Malignant Melanoma.Acta Dermatovenerol Croat. 2023 Dec;31(3):165-168. Acta Dermatovenerol Croat. 2023. PMID: 38439731
-
Melanocytic nevi simulant of melanoma with medicolegal relevance.Virchows Arch. 2007 Sep;451(3):623-47. doi: 10.1007/s00428-007-0459-7. Epub 2007 Jul 26. Virchows Arch. 2007. PMID: 17653760 Review.
-
Problematic lesions in children.Dermatol Clin. 2013 Oct;31(4):535-47, vii. doi: 10.1016/j.det.2013.06.003. Epub 2013 Jul 10. Dermatol Clin. 2013. PMID: 24075543 Review.
-
Clinical and histopathological features of pagetoid Spitz nevi of the thigh.J Cutan Pathol. 2020 Dec;47(12):1143-1149. doi: 10.1111/cup.13854. Epub 2020 Sep 8. J Cutan Pathol. 2020. PMID: 32829516
-
Atypical cellular blue nevi (cellular blue nevi with atypical features): lack of consensus for diagnosis and distinction from cellular blue nevi and malignant melanoma ("malignant blue nevus").Am J Surg Pathol. 2008 Jan;32(1):36-44. doi: 10.1097/PAS.0b013e3181573aaf. Am J Surg Pathol. 2008. PMID: 18162768
Cited by
-
Insights into Melanoma Clinical Practice: A Perspective for Future Research.Cancers (Basel). 2023 Sep 19;15(18):4631. doi: 10.3390/cancers15184631. Cancers (Basel). 2023. PMID: 37760601 Free PMC article.
-
Blue Nevus Associated With Acquired Dermal Melanocytosis on the Back.Cureus. 2024 Jul 26;16(7):e65428. doi: 10.7759/cureus.65428. eCollection 2024 Jul. Cureus. 2024. PMID: 39184650 Free PMC article.
-
Benign Nevi Mimicking Melanoma: A Diagnostic Dilemma.Cureus. 2024 Nov 30;16(11):e74821. doi: 10.7759/cureus.74821. eCollection 2024 Nov. Cureus. 2024. PMID: 39618769 Free PMC article. Review.
-
Deep Learning Approach to Classify Cutaneous Melanoma in a Whole Slide Image.Cancers (Basel). 2023 Mar 22;15(6):1907. doi: 10.3390/cancers15061907. Cancers (Basel). 2023. PMID: 36980793 Free PMC article.
-
Review of Non-Invasive Imaging Technologies for Cutaneous Melanoma.Biosensors (Basel). 2025 May 7;15(5):297. doi: 10.3390/bios15050297. Biosensors (Basel). 2025. PMID: 40422036 Free PMC article. Review.
References
-
- Malignant melanoma: skin cancer-diagnosis, prevention, and treatment. Ahmed B, Qadir MI, Ghafoor S. Crit Rev Eukaryot Gene Expr. 2020;30:291–297. - PubMed
-
- Gardner J. Arlington Virginia: Innovative Pathology Press; 2019. Survival Guide To Dermatopathology, Pathology Survival Guides Series 1.
-
- Cancer stat facts: melanoma of the skin. [ May; 2022 ];https://seer.cancer.gov/statfacts/html/melan.html 2022
Publication types
LinkOut - more resources
Full Text Sources