

Cervical Motor and Nociceptive Dysfunction After an Acute Whiplash Injury and the Association With Long-Term Non-Recovery: Revisiting a One-Year Prospective Cohort With Ankle Injured Controls
- PMID: 35875480
- PMCID: PMC9300940
- DOI: 10.3389/fpain.2022.906638
Cervical Motor and Nociceptive Dysfunction After an Acute Whiplash Injury and the Association With Long-Term Non-Recovery: Revisiting a One-Year Prospective Cohort With Ankle Injured Controls
Abstract
Aims: To explore the development of cervical motor and nociceptive dysfunction in patients with whiplash (WPs) and non-recovery based on injury-related work disability 1-year after injury when compared with ankle-injured controls (ACs).
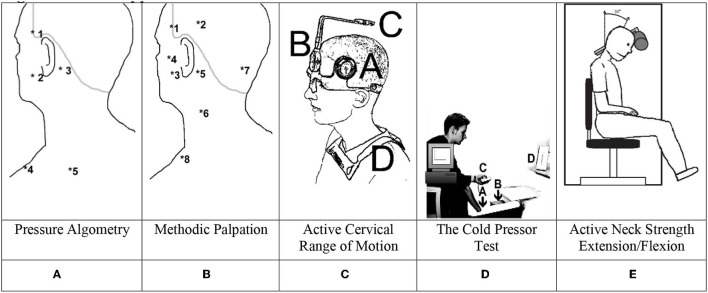
Methods: A 1-year observational prospective study examining consecutive WPs and age- and sex-matched ACs at 1 week,3 months, 6 months, and 1 year post-injury using semi-structured interviews; global pain rating (VAS0-10) and the pain rating index (PRI-T) and number-of-words-chosen (NWC) from the McGill Pain Questionnaire; examining nociceptive functioning using the cold pressor test (CPT), pressure algometry, and methodic palpation, and central pain processing using counter-stimulation; and examining motor functioning by active cervical range-of-motion (CROM), and neck strength [maximal voluntary contraction flexion/extension (MVC)]. One-year work disability/non-recovery was determined using a semi-structured interview.
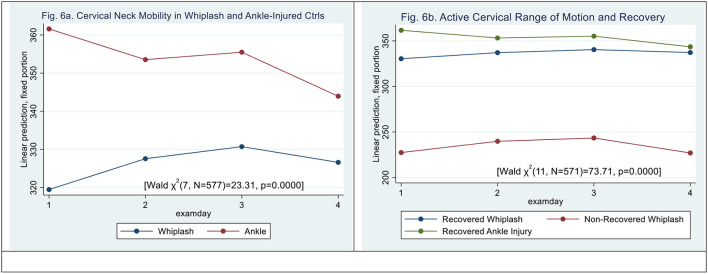
Results: A total of 141 WPs and 40 ACs were included. Total pain rating index (PRI-T) NWC were higher in ACs after 1 week but higher in WPs after 3 months, 6 months, and 1 year. Ongoing global pain was higher in WPs after 1 week and after 3 and 6 months but not after 1 year. Pressure pain thresholds were reduced, and palpation was higher in the neck and jaw in WPs after 1 week but was not consistently different afterward from ACs. Cervical mobility was reduced in WPs after 1 week, 3 months, and 6 months but not after 1 year, and MVC was significantly reduced in WPs when compared with ACs after 1 week and 1 year but not after 3 and 6 months. One-year non-recovery was only encountered in 11 WPs and not in the AC group. Non-recovered WPs (N-WPs) had consistently significantly higher VAS0-10, PRI-T, NWC, reduced pressure pain thresholds, raised muscle-tenderness, reduced active cervical range-of-motion, reduced active-neck-flexion/extension, and reported higher neck disability scores than recovered WPs. Of special interest, there was increasing tenderness in trigeminal-derived muscles based on palpation scores, and marked reduction of PPDT was most pronounced in N-WPs when compared with recovered WPs and ACs.
Conclusion: Cervical motor dysfunction and segmental nociceptive sensitization were present from early after injury in WPs and prolonged in N-WPs. Differences in trigeminal and cervical motor and sensory function in N-WPs could be of interest for future treatment studies.
Keywords: acute whiplash injury; control group; motor dysfunction; nociceptive dysfunction; prospective observational study.
Copyright © 2022 Kasch, Carstensen, Ravn, Andersen and Frostholm.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





Similar articles
-
Reduced cold pressor pain tolerance in non-recovered whiplash patients: a 1-year prospective study.Eur J Pain. 2005 Oct;9(5):561-9. doi: 10.1016/j.ejpain.2004.11.011. Epub 2004 Dec 30. Eur J Pain. 2005. PMID: 16139185
-
Whiplash injury results in sustained impairments of cervical muscle function: A one-year prospective, controlled study.J Rehabil Med. 2018 Jun 15;50(6):548-555. doi: 10.2340/16501977-2348. J Rehabil Med. 2018. PMID: 29767228
-
Pain thresholds and tenderness in neck and head following acute whiplash injury: a prospective study.Cephalalgia. 2001 Apr;21(3):189-97. doi: 10.1046/j.1468-2982.2001.00179.x. Cephalalgia. 2001. PMID: 11442553
-
Some observations on whiplash injuries.Neurol Clin. 1992 Nov;10(4):975-97. Neurol Clin. 1992. PMID: 1435666 Review.
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
References
-
- Walton DM, Carroll LJ, Kasch H, Sterling M, Verhagen AP, Macdermid JC, et al. . An overview of systematic reviews on prognostic factors in neck pain: results from the International Collaboration on Neck Pain (ICON) project. Open Orthop J. (2013) 7:494–505. 10.2174/1874325001307010494 - DOI - PMC - PubMed
-
- Holm LW, Carroll LJ, Cassidy JD, Hogg-Johnson S, Cote P, Guzman J, et al. . The burden and determinants of neck pain in whiplash-associated disorders after traffic collisions: results of the bone and joint decade 2000-2010 task force on neck pain and its associated disorders. J Manipulative Physiol Ther. (2009) 32:S61–9. 10.1016/j.jmpt.2008.11.011 - DOI - PubMed
LinkOut - more resources
Full Text Sources