

Subject-Specific 3D Models to Investigate the Influence of Rehabilitation Exercises and the Twisted Structure on Achilles Tendon Strains
- PMID: 35875495
- PMCID: PMC9299361
- DOI: 10.3389/fbioe.2022.914137
Subject-Specific 3D Models to Investigate the Influence of Rehabilitation Exercises and the Twisted Structure on Achilles Tendon Strains
Abstract
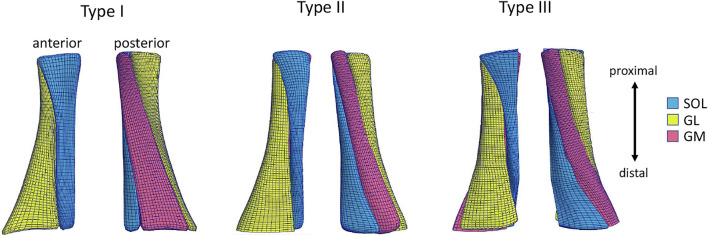
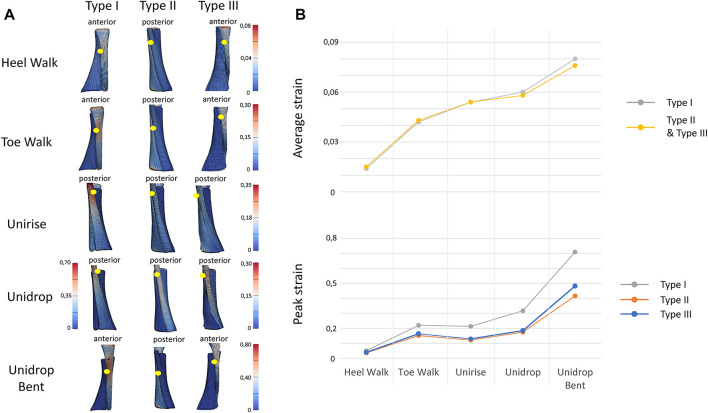
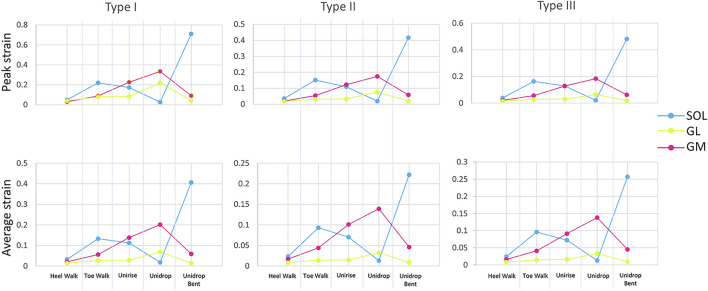
The Achilles tendon (AT) is the largest tendon of the human body and has a primary role in locomotor activities. The complex structure of the AT includes twisting of three sub-tendons, non-uniform tissue deformations and differential triceps surae muscle forces. The main aim of this study was to investigate the impact of commonly used rehabilitation exercises (walking on heels, walking on toes, unilateral heel rise, heel drop with extended knee and heel drop with the knee bent) and different twists on AT strains. 3D freehand ultrasound based subject-specific geometry and subject-specific muscle forces during different types of rehabilitation exercises were used to determine tendon strains magnitudes and differences in strains between the sub-tendons. In addition, three Finite Element models were developed to investigate the impact of AT twist. While walking on heels developed the lowest average strain, heel drop with knee bent exhibited the highest average strain. The eccentric heel drop resulted in higher peak and average strain, compared to concentric heel rise for all the three models. The isolated exercises (heel rise and heel drop) presented higher average strains compared to the functional exercises (walking tasks). The amount of twist influences the peak strains but not the average. Type I consistently showed highest peak strains among the five rehabilitation exercises. The ranking of the exercises based on the AT strains was independent of AT twist. These findings might help clinicians to prescribe rehabilitation exercises for Achilles tendinopathy based on their impact on the AT strains.
Keywords: achilles tendon; fascicle twist; finite element modeling; rehabilitation exercises; sub-tendon morphology; tendon strain.
Copyright © 2022 Funaro, Shim, Crouzier, Mylle and Vanwanseele.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources