

Effect of a Comprehensive Telehealth Intervention vs Telemonitoring and Care Coordination in Patients With Persistently Poor Type 2 Diabetes Control: A Randomized Clinical Trial
- PMID: 35877092
- PMCID: PMC9315987
- DOI: 10.1001/jamainternmed.2022.2947
Effect of a Comprehensive Telehealth Intervention vs Telemonitoring and Care Coordination in Patients With Persistently Poor Type 2 Diabetes Control: A Randomized Clinical Trial
Abstract
Importance: Persistently poorly controlled type 2 diabetes (PPDM) is common and causes poor outcomes. Comprehensive telehealth interventions could help address PPDM, but effectiveness is uncertain, and barriers impede use in clinical practice.
Objective: To address evidence gaps preventing use of comprehensive telehealth for PPDM by comparing a practical, comprehensive telehealth intervention to a simpler telehealth approach.
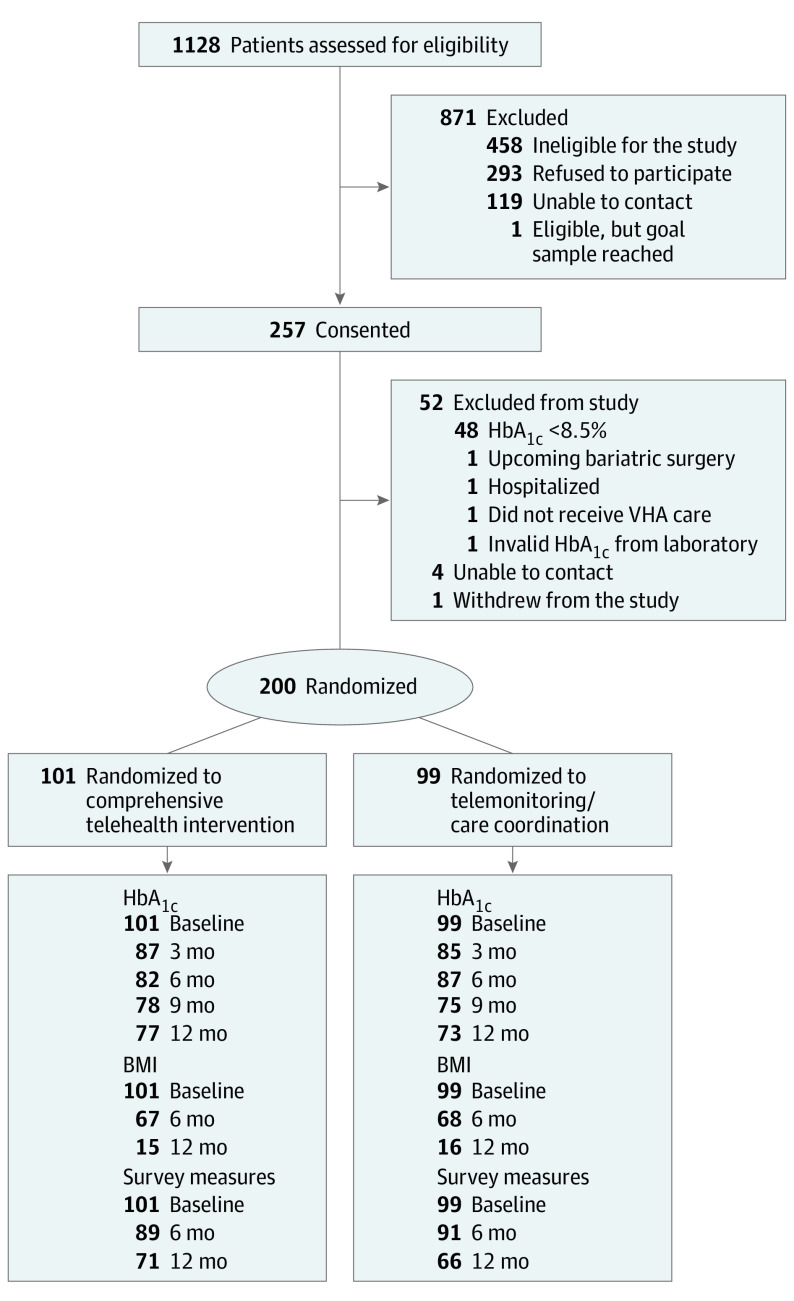
Design, setting, and participants: This active-comparator, parallel-arm, randomized clinical trial was conducted in 2 Veterans Affairs health care systems. From December 2018 to January 2020, 1128 outpatients with PPDM were assessed for eligibility and 200 were randomized; PPDM was defined as maintenance of hemoglobin A1c (HbA1c) level of 8.5% or higher for 1 year or longer despite engagement with clinic-based primary care and/or diabetes specialty care. Data analyses were preformed between March 2021 and May 2022.
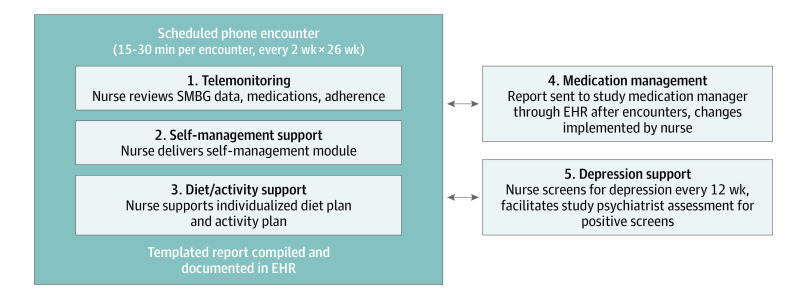
Interventions: Each 12-month intervention was nurse-delivered and used only clinical staffing/resources. The comprehensive telehealth group (n = 101) received telemonitoring, self-management support, diet/activity support, medication management, and depression support. Patients assigned to the simpler intervention (n = 99) received telemonitoring and care coordination.
Main outcomes and measures: Primary (HbA1c) and secondary outcomes (diabetes distress, diabetes self-care, self-efficacy, body mass index, depression symptoms) were analyzed over 12 months using intent-to-treat linear mixed longitudinal models. Sensitivity analyses with multiple imputation and inclusion of clinical data examined the impact of missing HbA1c measurements. Adverse events and intervention costs were examined.
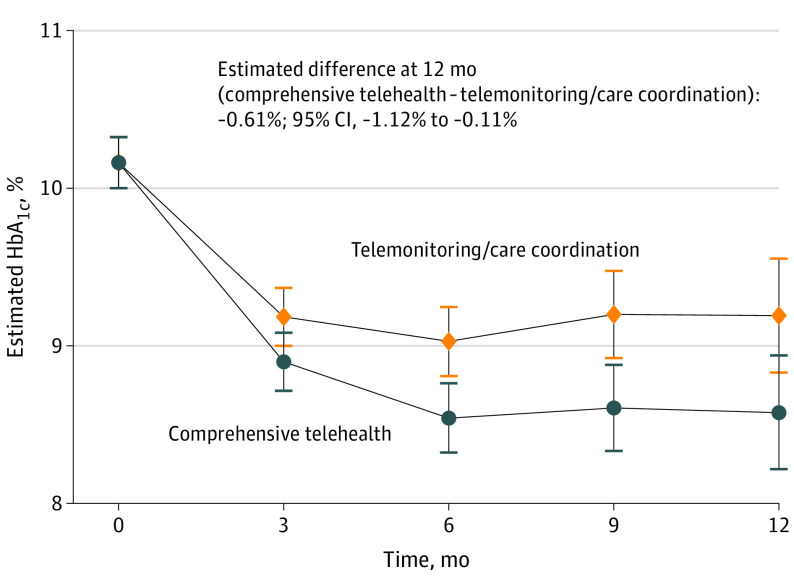
Results: The population (n = 200) had a mean (SD) age of 57.8 (8.2) years; 45 (22.5%) were women, 144 (72.0%) were of Black race, and 11 (5.5%) were of Hispanic/Latinx ethnicity. From baseline to 12 months, HbA1c change was -1.59% (10.17% to 8.58%) in the comprehensive telehealth group and -0.98% (10.17% to 9.19%) in the telemonitoring/care coordination group, for an estimated mean difference of -0.61% (95% CI, -1.12% to -0.11%; P = .02). Sensitivity analyses showed similar results. At 12 months, patients receiving comprehensive telehealth had significantly greater improvements in diabetes distress, diabetes self-care, and self-efficacy; no differences in body mass index or depression were seen. Adverse events were similar between groups. Comprehensive telehealth cost an additional $1519 per patient per year to deliver.
Conclusions and relevance: This randomized clinical trial found that compared with telemonitoring/care coordination, comprehensive telehealth improved multiple outcomes in patients with PPDM at a reasonable additional cost. This study supports consideration of comprehensive telehealth implementation for PPDM in systems with appropriate infrastructure and may enhance the value of telehealth during the COVID-19 pandemic and beyond.
Trial registration: ClinicalTrials.gov Identifier: NCT03520413.
Conflict of interest statement
Figures
References
-
- Kobe EA, Edelman D, Tarkington PE, et al. Practical telehealth to improve control and engagement for patients with clinic-refractory diabetes mellitus (PRACTICE-DM): protocol and baseline data for a randomized trial. Contemp Clin Trials. 2020;98:106157. doi: 10.1016/j.cct.2020.106157 - DOI - PMC - PubMed
