

Effects of Pulsatile Flow Rate and Shunt Ratio in Bifurcated Distal Arteries on Hemodynamic Characteristics Involved in Two Patient-Specific Internal Carotid Artery Sidewall Aneurysms: A Numerical Study
- PMID: 35877376
- PMCID: PMC9311626
- DOI: 10.3390/bioengineering9070326
Effects of Pulsatile Flow Rate and Shunt Ratio in Bifurcated Distal Arteries on Hemodynamic Characteristics Involved in Two Patient-Specific Internal Carotid Artery Sidewall Aneurysms: A Numerical Study
Abstract
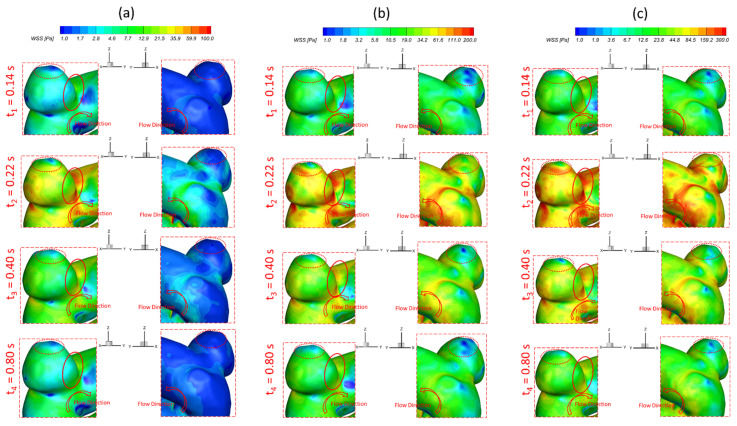
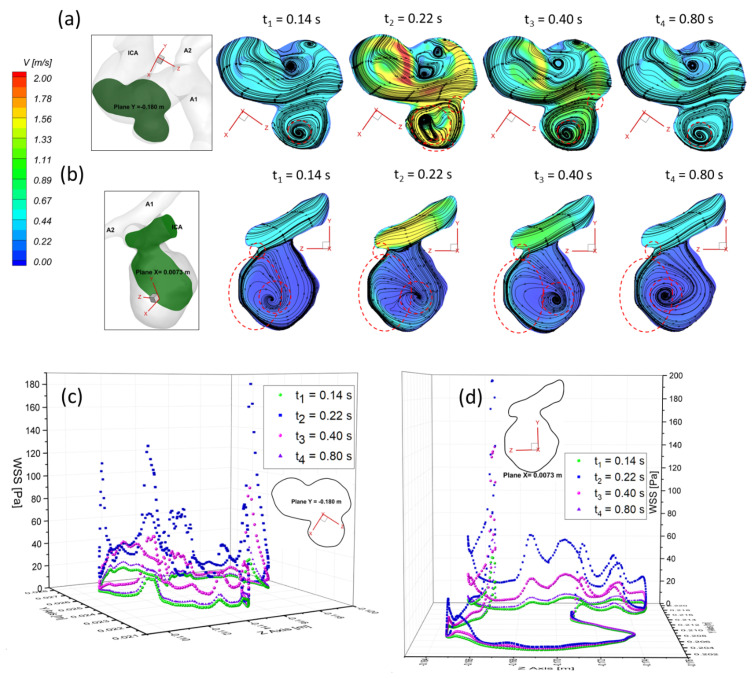
The pulsatile flow rate (PFR) in the cerebral artery system and shunt ratios in bifurcated arteries are two patient-specific parameters that may affect the hemodynamic characteristics in the pathobiology of cerebral aneurysms, which needs to be identified comprehensively. Accordingly, a systematic study was employed to study the effects of pulsatile flow rate (i.e., PFR-I, PFR-II, and PFR-III) and shunt ratio (i.e., 75:25 and 64:36) in bifurcated distal arteries, and transient cardiac pulsatile waveform on hemodynamic patterns in two internal carotid artery sidewall aneurysm models using computational fluid dynamics (CFD) modeling. Numerical results indicate that larger PFRs can cause higher wall shear stress (WSS) in some local regions of the aneurysmal dome that may increase the probability of small/secondary aneurysm generation than under smaller PFRs. The low WSS and relatively high oscillatory shear index (OSI) could appear under a smaller PFR, increasing the potential risk of aneurysmal sac growth and rupture. However, the variances in PFRs and bifurcated shunt ratios have rare impacts on the time-average pressure (TAP) distributions on the aneurysmal sac, although a higher PFR can contribute more to the pressure increase in the ICASA-1 dome due to the relatively stronger impingement by the redirected bloodstream than in ICASA-2. CFD simulations also show that the variances of shunt ratios in bifurcated distal arteries have rare impacts on the hemodynamic characteristics in the sacs, mainly because the bifurcated location is not close enough to the sac in present models. Furthermore, it has been found that the vortex location plays a major role in the temporal and spatial distribution of the WSS on the luminal wall, varying significantly with the cardiac period.
Keywords: bifurcated shunt ratio; computational fluid dynamics (CFD); hemodynamic behaviors; internal carotid artery sidewall aneurysm (ICASA); oscillatory shear index (OSI); pulsatile flow rate (PFR); time-averaged pressure (TAP); wall shear stress (WSS).
Conflict of interest statement
The authors have no conflict to disclose.
Figures











Similar articles
-
Developing an in vitro validated 3D in silico internal carotid artery sidewall aneurysm model.Front Physiol. 2022 Dec 20;13:1024590. doi: 10.3389/fphys.2022.1024590. eCollection 2022. Front Physiol. 2022. PMID: 36605897 Free PMC article.
-
Newtonian viscosity model could overestimate wall shear stress in intracranial aneurysm domes and underestimate rupture risk.J Neurointerv Surg. 2012 Sep;4(5):351-7. doi: 10.1136/neurintsurg-2011-010089. Epub 2011 Sep 19. J Neurointerv Surg. 2012. PMID: 21990529
-
Hemodynamic and morphological characteristics of a growing cerebral aneurysm.Neurosurg Focus. 2019 Jul 1;47(1):E13. doi: 10.3171/2019.4.FOCUS19195. Neurosurg Focus. 2019. PMID: 31261117 Free PMC article.
-
Computational fluid dynamics as a risk assessment tool for aneurysm rupture.Neurosurg Focus. 2019 Jul 1;47(1):E12. doi: 10.3171/2019.4.FOCUS19189. Neurosurg Focus. 2019. PMID: 31261116 Review.
-
A comparison of 4D flow MRI-derived wall shear stress with computational fluid dynamics methods for intracranial aneurysms and carotid bifurcations - A review.Magn Reson Imaging. 2018 May;48:62-69. doi: 10.1016/j.mri.2017.12.005. Epub 2017 Dec 6. Magn Reson Imaging. 2018. PMID: 29223732 Review.
Cited by
-
Evaluation of hemodynamic effects of different inferior vena cava filter heads using computational fluid dynamics.Front Bioeng Biotechnol. 2022 Oct 10;10:1034120. doi: 10.3389/fbioe.2022.1034120. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 36299290 Free PMC article.
-
Hemodynamic characteristics in a cerebral aneurysm model using non-Newtonian blood analogues.Phys Fluids (1994). 2022 Oct;34(10):103101. doi: 10.1063/5.0118097. Epub 2022 Oct 3. Phys Fluids (1994). 2022. PMID: 36212224 Free PMC article.
-
Developing an in vitro validated 3D in silico internal carotid artery sidewall aneurysm model.Front Physiol. 2022 Dec 20;13:1024590. doi: 10.3389/fphys.2022.1024590. eCollection 2022. Front Physiol. 2022. PMID: 36605897 Free PMC article.
-
Morphology and Hemodynamics of Cerebral Arteries and Aneurysms in a Rare Pair of Monozygotic Twins.Diagnostics (Basel). 2023 Jun 8;13(12):2004. doi: 10.3390/diagnostics13122004. Diagnostics (Basel). 2023. PMID: 37370899 Free PMC article.
-
Machine Learning for Aiding Blood Flow Velocity Estimation Based on Angiography.Bioengineering (Basel). 2022 Oct 28;9(11):622. doi: 10.3390/bioengineering9110622. Bioengineering (Basel). 2022. PMID: 36354533 Free PMC article.
References
-
- Moossy J. Pathology of the Cerebral Blood Vessels. Arch. Neurol. 1973;28:284. doi: 10.1001/archneur.1973.00490220092021. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
