

The potential of a nomogram combined PI-RADS v2.1 and contrast-enhanced ultrasound (CEUS) to reduce unnecessary biopsies in prostate cancer diagnostics
- PMID: 35877385
- PMCID: PMC9815734
- DOI: 10.1259/bjr.20220209
The potential of a nomogram combined PI-RADS v2.1 and contrast-enhanced ultrasound (CEUS) to reduce unnecessary biopsies in prostate cancer diagnostics
Abstract
Objectives: To develop a nomogram prediction model based on Prostate Imaging Reporting and Data System v.2.1 (PI-RADS v2.1) and contrast-enhanced ultrasound (CEUS) for predicting prostate cancer (PCa) and clinically significant prostate cancer (csPCa) in males with prostate-specific antigen (PSA) 4-10 ng ml-1 to avoid unnecessary biopsy.
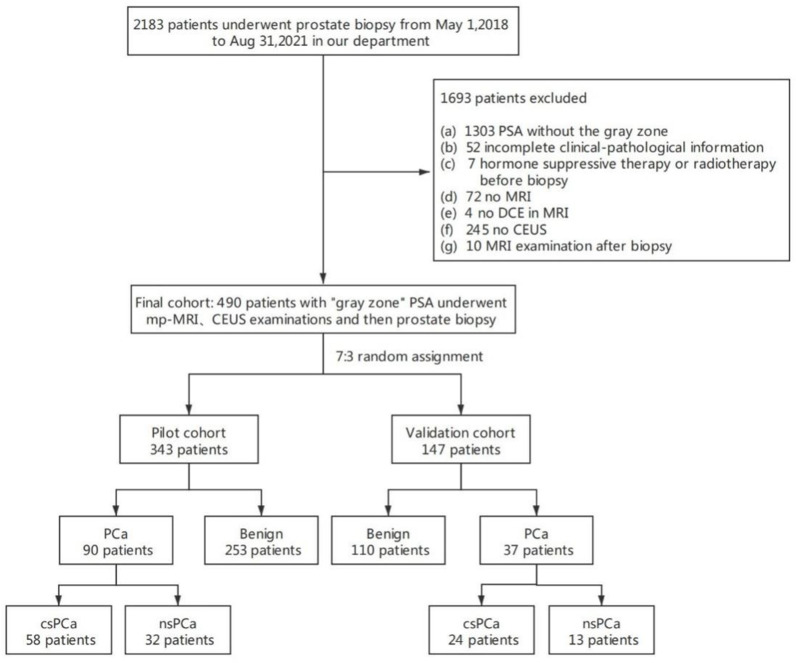
Methods: A total of 490 patients who underwent prostate biopsy for PSA 4-10 ng ml-1 were enrolled and randomly divided into a pilot cohort (70%) and a validation cohort (30%). Univariate and multivariate logistic regression models were constructed to select potential predictors of PCa and csPCa, and a nomogram was created. The area under receiver operating characteristic (ROC) curve (AUC) was calculated, and compared using DeLong's test. The diagnostic performance and unnecessary biopsy rate of the nomogram prediction model were also assessed. Hosmer-Lemeshow goodness-of-fit test was employed to test for model fitness.
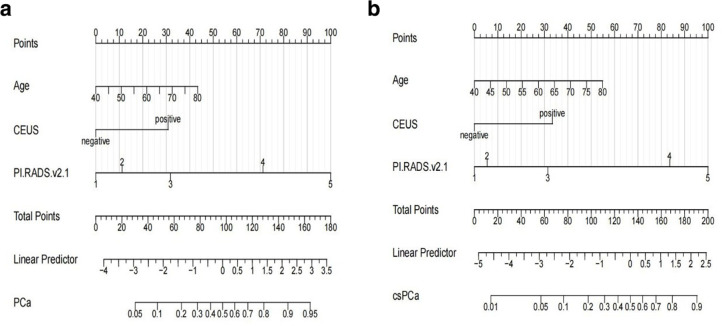
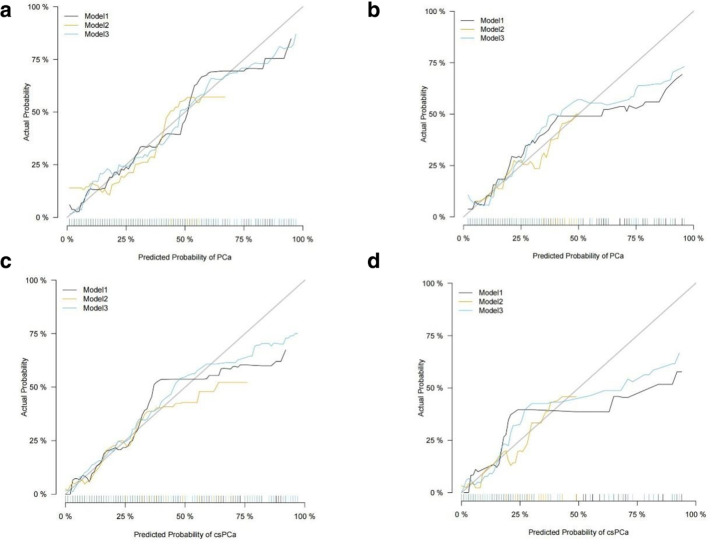
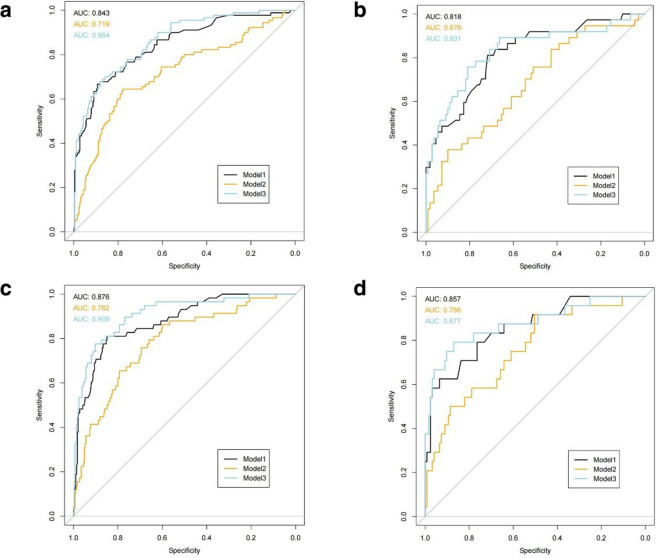
Results: The multivariate analysis revealed that features independently associated with PCa and csPCa were age, PI-RADS score and CEUS manifestations. Incorporating these factors, the nomogram achieved good discrimination performance of AUC 0.843 for PCa, 0.876 for csPCa in the pilot cohort, and 0.818 for PCa, 0.857 for csPCa in the validation cohort, respectively, and had well-fitted calibration curves. And the diagnostic performance of the nomogram was comparable to the model including all the parameters (p > 0.05). Besides, the nomogram prediction model yielded meaningful reduction in unnecessary biopsy rate (from 74.8 to 21.1% in PCa, and from 83.7 to 5.4% in csPCa).
Conclusions: The nomogram prediction model based on age, PI-RADS v2.1 and CEUS achieved an optimal prediction of PCa and csPCa. Using this model, the PCa risk for an individual patient can be estimated, which can lead to a rational biopsy choice.
Advances in knowledge: This study gives an account of improving pre-biopsy risk stratification in males with "gray zone" PSA level through PI-RADS v2.1 and CEUS.
Conflict of interest statement
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
