

Multimodal Registration for Image-Guided EBUS Bronchoscopy
- PMID: 35877633
- PMCID: PMC9320860
- DOI: 10.3390/jimaging8070189
Multimodal Registration for Image-Guided EBUS Bronchoscopy
Abstract
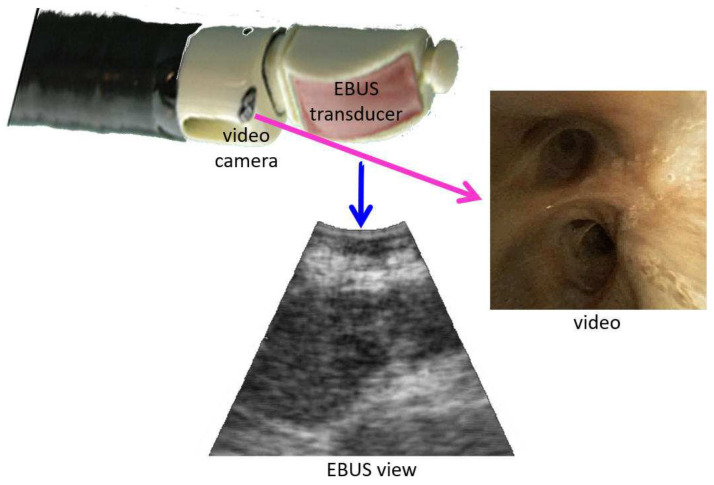
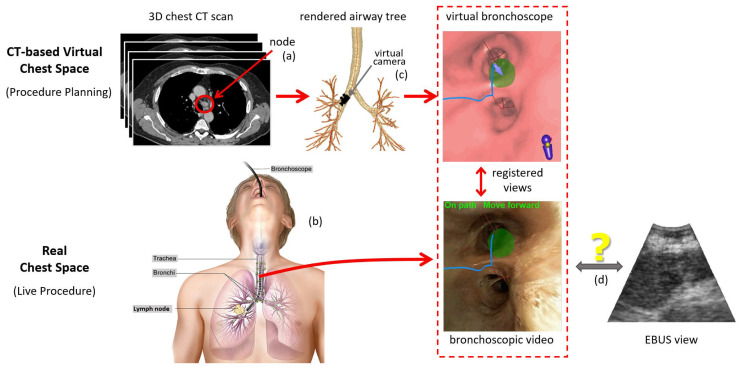
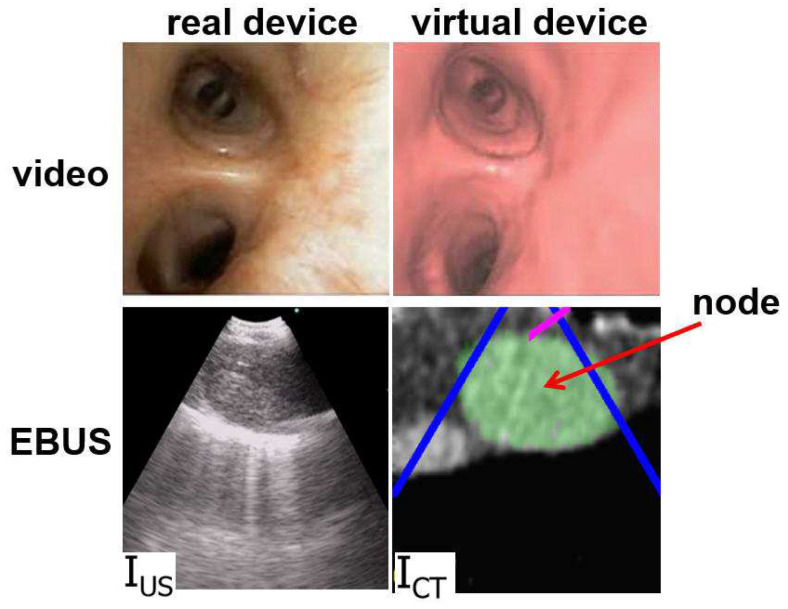
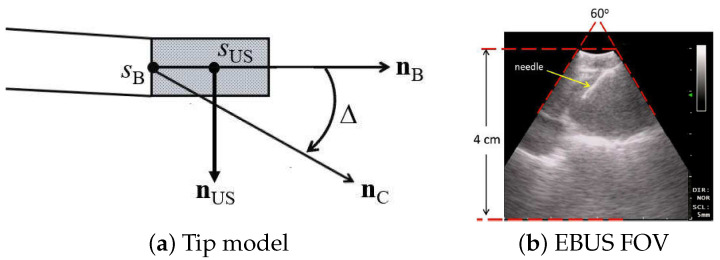
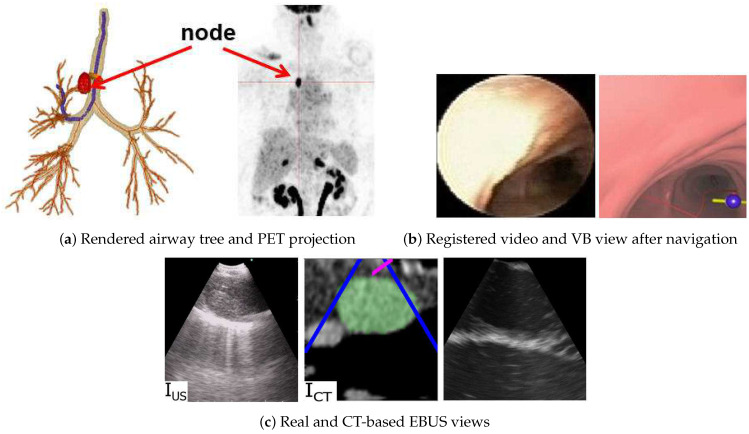
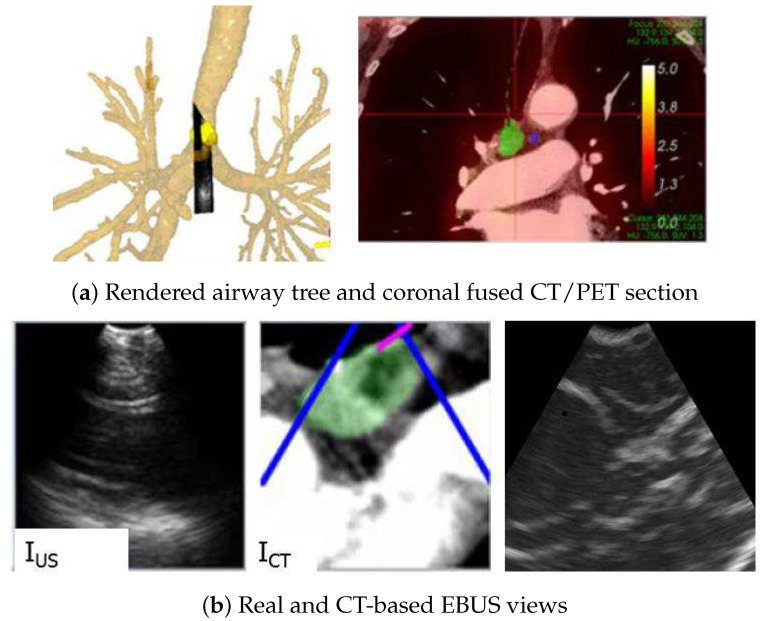
The state-of-the-art procedure for examining the lymph nodes in a lung cancer patient involves using an endobronchial ultrasound (EBUS) bronchoscope. The EBUS bronchoscope integrates two modalities into one device: (1) videobronchoscopy, which gives video images of the airway walls; and (2) convex-probe EBUS, which gives 2D fan-shaped views of extraluminal structures situated outside the airways. During the procedure, the physician first employs videobronchoscopy to navigate the device through the airways. Next, upon reaching a given node's approximate vicinity, the physician probes the airway walls using EBUS to localize the node. Due to the fact that lymph nodes lie beyond the airways, EBUS is essential for confirming a node's location. Unfortunately, it is well-documented that EBUS is difficult to use. In addition, while new image-guided bronchoscopy systems provide effective guidance for videobronchoscopic navigation, they offer no assistance for guiding EBUS localization. We propose a method for registering a patient's chest CT scan to live surgical EBUS views, thereby facilitating accurate image-guided EBUS bronchoscopy. The method entails an optimization process that registers CT-based virtual EBUS views to live EBUS probe views. Results using lung cancer patient data show that the method correctly registered 28/28 (100%) lymph nodes scanned by EBUS, with a mean registration time of 3.4 s. In addition, the mean position and direction errors of registered sites were 2.2 mm and 11.8∘, respectively. In addition, sensitivity studies show the method's robustness to parameter variations. Lastly, we demonstrate the method's use in an image-guided system designed for guiding both phases of EBUS bronchoscopy.
Keywords: bronchoscopy; endobronchial ultrasound; image registration; image-guided surgery systems; lung cancer; multimodal imaging.
Conflict of interest statement
William E. Higgins and Penn State have an identified conflict of interest and financial interest related to this research. These interests have been reviewed by the University’s Institutional and Individual Conflict of Interest Committees and are currently being managed by the University and reported to the NIH.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
