

Blood pressure-lowering treatment for prevention of major cardiovascular diseases in people with and without type 2 diabetes: an individual participant-level data meta-analysis
- PMID: 35878651
- PMCID: PMC9622419
- DOI: 10.1016/S2213-8587(22)00172-3
Blood pressure-lowering treatment for prevention of major cardiovascular diseases in people with and without type 2 diabetes: an individual participant-level data meta-analysis
Abstract
Background: Controversy exists as to whether the threshold for blood pressure-lowering treatment should differ between people with and without type 2 diabetes. We aimed to investigate the effects of blood pressure-lowering treatment on the risk of major cardiovascular events by type 2 diabetes status, as well as by baseline levels of systolic blood pressure.
Methods: We conducted a one-stage individual participant-level data meta-analysis of major randomised controlled trials using the Blood Pressure Lowering Treatment Trialists' Collaboration dataset. Trials with information on type 2 diabetes status at baseline were eligible if they compared blood pressure-lowering medications versus placebo or other classes of blood pressure-lowering medications, or an intensive versus a standard blood pressure-lowering strategy, and reported at least 1000 persons-years of follow-up in each group. Trials exclusively on participants with heart failure or with short-term therapies and acute myocardial infarction or other acute settings were excluded. We expressed treatment effect per 5 mm Hg reduction in systolic blood pressure on the risk of developing a major cardiovascular event as the primary outcome, defined as the first occurrence of fatal or non-fatal stroke or cerebrovascular disease, fatal or non-fatal ischaemic heart disease, or heart failure causing death or requiring hospitalisation. Cox proportional hazard models, stratified by trial, were used to estimate hazard ratios (HRs) separately by type 2 diabetes status at baseline, with further stratification by baseline categories of systolic blood pressure (in 10 mm Hg increments from <120 mm Hg to ≥170 mm Hg). To estimate absolute risk reductions, we used a Poisson regression model over the follow-up duration. The effect of each of the five major blood pressure-lowering drug classes, including angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, β blockers, calcium channel blockers, and thiazide diuretics, was estimated using a network meta-analysis framework. This study is registered with PROSPERO, CRD42018099283.
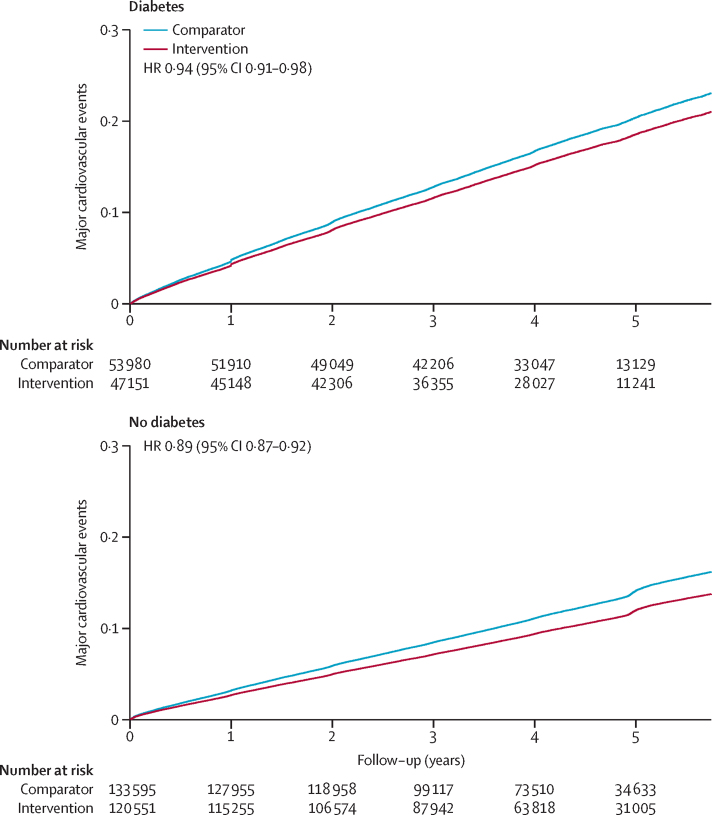
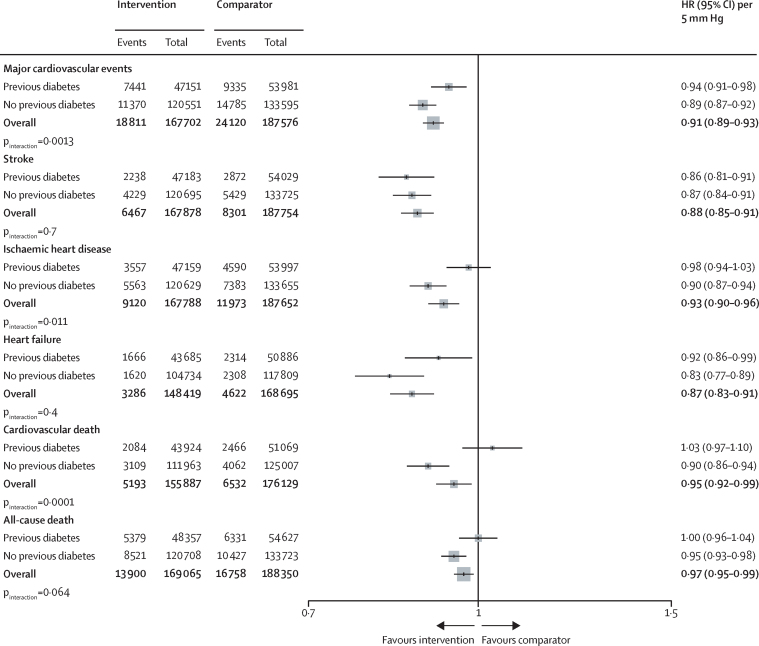
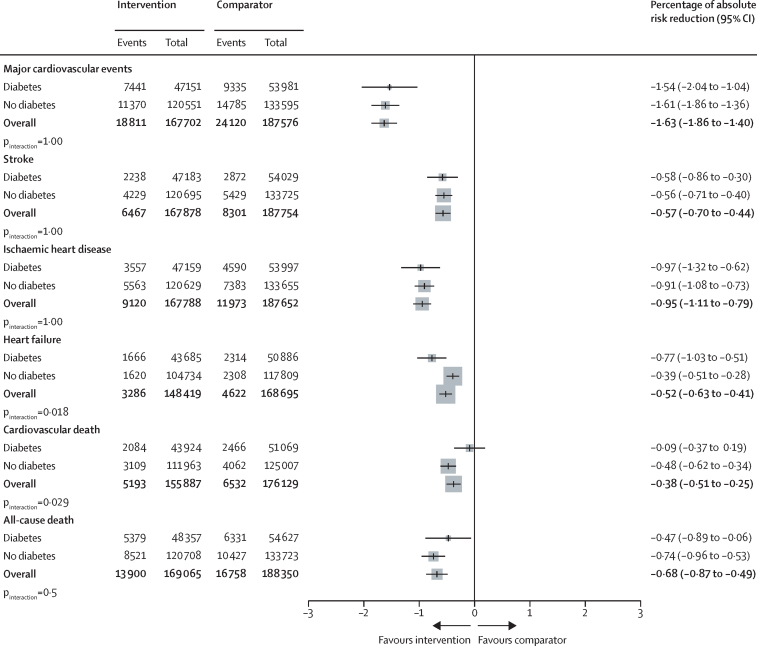
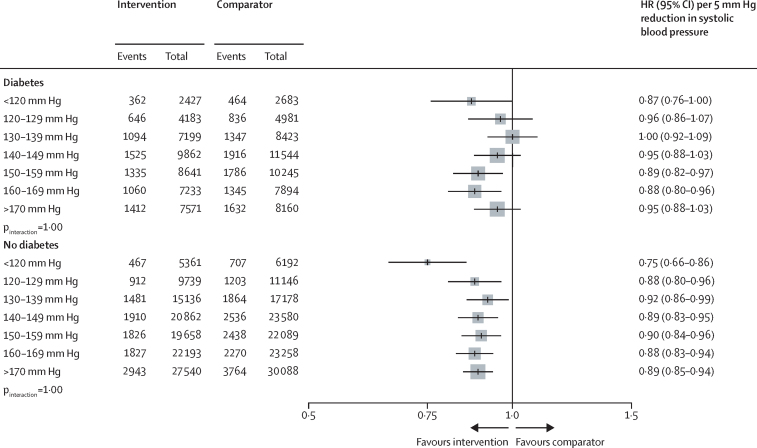
Findings: We included data from 51 randomised clinical trials published between 1981 and 2014 involving 358 533 participants (58% men), among whom 103 325 (29%) had known type 2 diabetes at baseline. The baseline mean systolic/diastolic blood pressure of those with and without type 2 diabetes was 149/84 mm Hg (SD 19/11) and 153/88 mm Hg (SD 21/12), respectively. Over 4·2 years median follow-up (IQR 3·0-5·0), a 5 mm Hg reduction in systolic blood pressure decreased the risk of major cardiovascular events in both groups, but with a weaker relative treatment effect in participants with type 2 diabetes (HR 0·94 [95% CI 0·91-0·98]) compared with those without type 2 diabetes (0·89 [0·87-0·92]; pinteraction=0·0013). However, absolute risk reductions did not differ substantially between people with and without type 2 diabetes because of the higher absolute cardiovascular risk among participants with type 2 diabetes. We found no reliable evidence for heterogeneity of treatment effects by baseline systolic blood pressure in either group. In keeping with the primary findings, analysis using stratified network meta-analysis showed no evidence that relative treatment effects differed substantially between participants with type 2 diabetes and those without for any of the drug classes investigated.
Interpretation: Although the relative beneficial effects of blood pressure reduction on major cardiovascular events were weaker in participants with type 2 diabetes than in those without, absolute effects were similar. The difference in relative risk reduction was not related to the baseline blood pressure or allocation to different drug classes. Therefore, the adoption of differential blood pressure thresholds, intensities of blood pressure lowering, or drug classes used in people with and without type 2 diabetes is not warranted.
Funding: British Heart Foundation, UK National Institute for Health Research, and Oxford Martin School.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests KR reports personal fees from the BMJ Heart and PLOS Medicine, outside of the submitted work. MW reports personal funding from Amgen, Kyowa Kirin, and Freeline, outside of the current work. NS has consulted for, or received lecture fees from, Afimmune, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Hanmi Pharmaceuticals, MSD, Novartis, Novo Nordisk, Pfizer, and Sanofi; and received grant support from AstraZeneca, Boehringer Ingelheim, Novartis, and Roche Diagnostics through his institution, the University of Glasgow. RRH reports research support from AstraZeneca, Bayer, and MSD; and personal fees from Anji Pharmaceuticals, Bayer, Novartis, and Novo Nordisk. RJM received blood pressure monitors from Omron for research and his institution receives fees from Omron and Sensyne for blood pressure telemonitoring systems. JC reports research grants and personal fees from Servier for the ADVANCE and PROGRESS trials, and grants from the National Health and Medical Research Council of Australia for these two trials. All other authors declare no competing interests.
Figures
Comment in
-
Blood pressure control according to type 2 diabetes status.Lancet Diabetes Endocrinol. 2022 Sep;10(9):612-613. doi: 10.1016/S2213-8587(22)00191-7. Epub 2022 Jul 22. Lancet Diabetes Endocrinol. 2022. PMID: 35878652 No abstract available.
-
Blood pressure reduction and major cardiovascular events in people with and without type 2 diabetes.Lancet Diabetes Endocrinol. 2022 Dec;10(12):840. doi: 10.1016/S2213-8587(22)00312-6. Lancet Diabetes Endocrinol. 2022. PMID: 36427519 No abstract available.
-
Blood pressure reduction and major cardiovascular events in people with and without type 2 diabetes.Lancet Diabetes Endocrinol. 2022 Dec;10(12):840-841. doi: 10.1016/S2213-8587(22)00311-4. Lancet Diabetes Endocrinol. 2022. PMID: 36427520 No abstract available.
-
Blood pressure reduction and major cardiovascular events in people with and without type 2 diabetes - Authors' reply.Lancet Diabetes Endocrinol. 2022 Dec;10(12):841-842. doi: 10.1016/S2213-8587(22)00310-2. Lancet Diabetes Endocrinol. 2022. PMID: 36427521 No abstract available.
-
BP-lowering drugs reduced major CV events by similar amounts in patients with and without type 2 diabetes.Ann Intern Med. 2022 Dec;175(12):JC138. doi: 10.7326/J22-0093. Epub 2022 Dec 6. Ann Intern Med. 2022. PMID: 36469918
References
-
- Emdin CA, Rahimi K, Neal B, Callender T, Perkovic V, Patel A. Blood pressure lowering in type 2 diabetes: a systematic review and meta-analysis. JAMA. 2015;313:603–615. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- FS/19/36/34346/BHF_/British Heart Foundation/United Kingdom
- MC_UU_00011/1/MRC_/Medical Research Council/United Kingdom
- PG/18/65/33872/BHF_/British Heart Foundation/United Kingdom
- MC_EX_G0801669/MRC_/Medical Research Council/United Kingdom
- MC_U137686849/MRC_/Medical Research Council/United Kingdom
- MC_UU_12026/6/MRC_/Medical Research Council/United Kingdom
- MR/S019669/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_00017/4/MRC_/Medical Research Council/United Kingdom
- CH/1996001/9454/BHF_/British Heart Foundation/United Kingdom
- MC_PC_12027/MRC_/Medical Research Council/United Kingdom
- MC_U137686854/MRC_/Medical Research Council/United Kingdom
- MC_PC_12029/MRC_/Medical Research Council/United Kingdom
- G0300622/MRC_/Medical Research Council/United Kingdom
- MC_PC_12028/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
