

Cancer Prevention with Resistant Starch in Lynch Syndrome Patients in the CAPP2-Randomized Placebo Controlled Trial: Planned 10-Year Follow-up
- PMID: 35878732
- PMCID: PMC9433960
- DOI: 10.1158/1940-6207.CAPR-22-0044
Cancer Prevention with Resistant Starch in Lynch Syndrome Patients in the CAPP2-Randomized Placebo Controlled Trial: Planned 10-Year Follow-up
Abstract
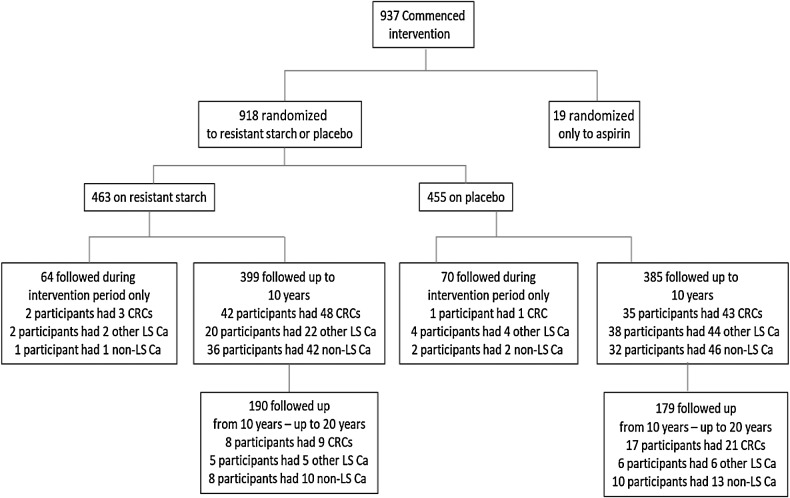
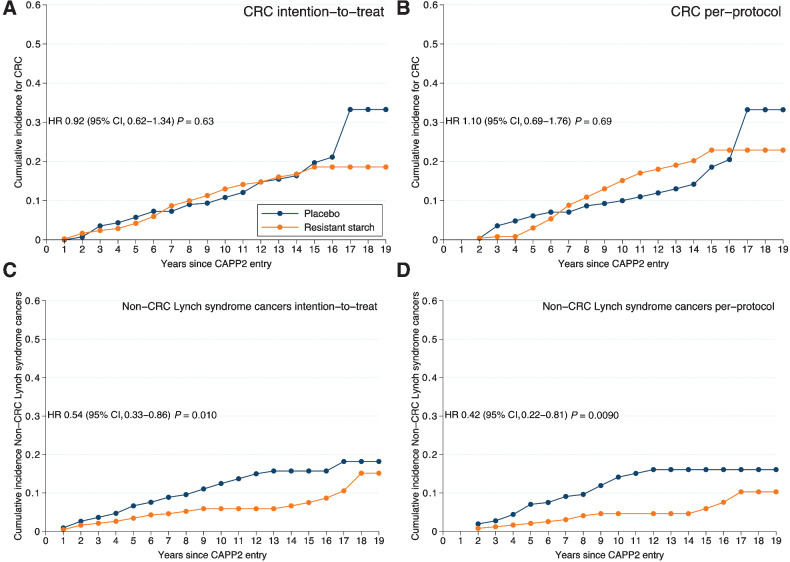
Abstract: The CAPP2 trial investigated the long-term effects of aspirin and resistant starch on cancer incidence in patients with Lynch syndrome (LS). Participants with LS were randomized double-blind to 30 g resistant starch (RS) daily or placebo for up to 4 years. We present long-term cancer outcomes based on the planned 10-year follow-up from recruitment, supplemented by National Cancer Registry data to 20 years in England, Wales, and Finland. Overall, 463 participants received RS and 455 participants received placebo. After up to 20 years follow-up, there was no difference in colorectal cancer incidence (n = 52 diagnosed with colorectal cancer among those randomized to RS against n = 53 on placebo) but fewer participants had non-colorectal LS cancers in those randomized to RS (n = 27) compared with placebo (n = 48); intention-to-treat (ITT) analysis [HR, 0.54; 95% confidence interval (CI), 0.33-0.86; P = 0.010]. In ITT analysis, allowing for multiple primary cancer diagnoses among participants by calculating incidence rate ratios (IRR) confirmed the protective effect of RS against non-colorectal cancer LS cancers (IRR, 0.52; 95% CI, 0.32-0.84; P = 0.0075). These effects are particularly pronounced for cancers of the upper GI tract; 5 diagnoses in those on RS versus 21 diagnoses on placebo. The reduction in non-colorectal cancer LS cancers was detectable in the first 10 years and continued in the next decade. For colorectal cancer, ITT analysis showed no effect of RS on colorectal cancer risk (HR, 0.92; 95% CI, 0.62-1.34; P = 0.63). There was no interaction between aspirin and RS treatments. In conclusion, 30 g daily RS appears to have a substantial protective effect against non-colorectal cancer cancers for patients with LS.
Prevention relevance: Regular bowel screening and aspirin reduce colorectal cancer among patients with LS but extracolonic cancers are difficult to detect and manage. This study suggests that RS reduces morbidity associated with extracolonic cancers. See related Spotlight, p. 557.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
-
Can a Banana a Day Keep the Cancer Away in Patients with Lynch Syndrome?Cancer Prev Res (Phila). 2022 Sep 1;15(9):557-559. doi: 10.1158/1940-6207.CAPR-22-0312. Cancer Prev Res (Phila). 2022. PMID: 36047056
-
CAPP2 RCT: Resistant Starch Planned Long-term Follow-up-Letter.Cancer Prev Res (Phila). 2023 Jan 4;16(1):57. doi: 10.1158/1940-6207.CAPR-22-0411. Cancer Prev Res (Phila). 2023. PMID: 36597729 No abstract available.
References
-
- Colorectal cancer NICE guideline [NG151] Published: 29 January 2020. [cited 2022 June 22]. Available from: https://www.nice.org.uk/guidance/NG151.
-
- Burkitt DP, Walker AR, Painter NS. Effect of dietary fibre on stools and the transit-times, and its role in the causation of disease. Lancet 1972;2:1408–12. - PubMed
-
- Park Y, Hunter DJ, Spiegelman D, Bergkvist L, Berrino F, van den Brandt PA, et al. Dietary fiber intake and risk of colorectal cancera pooled analysis of prospective cohort studies. JAMA 2005;294:2849–57. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
