

Single-Level Total Disc Replacement: Index-Level and Adjacent-Level Revision Surgery Incidence, Characteristics, and Outcomes
- PMID: 35878906
- PMCID: PMC10151392
- DOI: 10.14444/8331
Single-Level Total Disc Replacement: Index-Level and Adjacent-Level Revision Surgery Incidence, Characteristics, and Outcomes
Abstract
Background: The literature reports that index level (IL) revision spine surgery (RSS) and adjacent level (AL) RSS are diminished in lumbar TDR compared with fusion procedures. There is a paucity of PROMs reported after RSS.
Objective: To present the incidence of RSS at the IL and AL following single-level lumbar total disc replacement (TDR) and to document patient-related outcome measures (PROMs) associated with RSS.
Methods: PROMs and timelines were analyzed for 32 RSS patients from a prospective cohort study of 401 patients treated with TDR for single-level degenerative disc disease. The data collected prospectively are analyzed from baseline (prior to index surgery) to latest follow-up following RSS. PROMs, including visual analog scales for back and leg, Oswestry Disability Index, and Roland-Morris Disability Questionnaire, were collected preoperatively; postoperatively at 3, 6, and 12 months; and annually thereafter until RSS. The time to RSS was recorded, and PROMs for RSS (IL, AL, or both) were documented, analyzed, and compared.
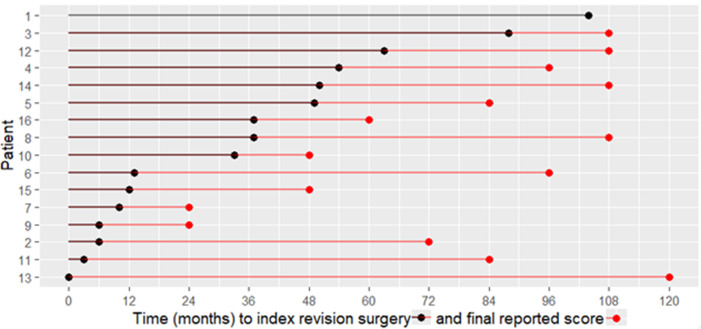
Results: The median time to RSS in the IL cohort was 35 months (interquartile range [IQR] = 9-51 months). The median time to RSS cohort was 70 months (IQR = 41.3-105.3 months). Timepoints facilitate PROM discussion for RSS. Patients in both groups achieved thresholds for the minimum clinically important difference for pain and disability scores. The small sample size in each group contributed to the variability demonstrated by the 95% CIs, thereby cautioning definitive conclusions.
Conclusions: This study reveals that statistically significant and modest clinical improvements in PROMs can be achieved in RSS for lumbar TDR at IL and AL. The surgical approach and technique are reflective of the pathology and suggest that anterior RSS for AL degeneration and posterior RSS for IL pathology yield similar results.
Clinical relevance: Statistical and clinical improvements can be achieved in IL-RSS and AL-RSS following single level TDR. It is essential for clinicians to understand and verify the underlying IL and/or AL pathology to select an appropriate management strategy and to facilitate balanced informed discussions with patients.
Keywords: adjacent segment; arthroplasty; artificial disc; back pain; degenerative disc disease; index level; long-term results; lumbar spine; motion preservation; revision; total disc replacement.
This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
Conflict of interest statement
Declaration of Conflicting Interests: Matthew Scott-Young previously received royalties and had a consulting agreement with DePuy Spine. The remaining authors report no disclosures.
Figures





Similar articles
-
Single-Level Total Disc Replacement: Mid- to Long-Term Outcomes.Int J Spine Surg. 2022 Jul 25;16(5):837-46. doi: 10.14444/8330. Online ahead of print. Int J Spine Surg. 2022. PMID: 35878907 Free PMC article.
-
Mid- to long-term results of total lumbar disc replacement: a prospective analysis with 5- to 10-year follow-up.Spine J. 2014 Aug 1;14(8):1417-31. doi: 10.1016/j.spinee.2013.08.028. Epub 2014 Jan 18. Spine J. 2014. PMID: 24448028
-
Motion preservation following total lumbar disc replacement at the lumbosacral junction: a prospective long-term clinical and radiographic investigation.Spine J. 2018 Jan;18(1):72-80. doi: 10.1016/j.spinee.2017.06.035. Epub 2017 Jun 30. Spine J. 2018. PMID: 28673830 Clinical Trial.
-
Comparison of Mid- to Long-term Follow-up of Patient-reported Outcomes Measures After Single-level Lumbar Total Disc Arthroplasty, Multi-level Lumbar Total Disc Arthroplasty, and the Lumbar Hybrid Procedure for the Treatment of Degenerative Disc Disease.Spine (Phila Pa 1976). 2022 Mar 1;47(5):377-386. doi: 10.1097/BRS.0000000000004253. Spine (Phila Pa 1976). 2022. PMID: 34559766 Free PMC article.
-
Mid- to long-term results of total disc replacement for lumbar degenerative disc disease: a systematic review.J Orthop Surg Res. 2018 Dec 26;13(1):326. doi: 10.1186/s13018-018-1032-6. J Orthop Surg Res. 2018. PMID: 30585142 Free PMC article.
Cited by
-
The Future of Arthroplasty in the Spine.Int J Spine Surg. 2025 Apr 7;19(S2):S25-S37. doi: 10.14444/8737. Int J Spine Surg. 2025. PMID: 40068878 Free PMC article.
-
Patient outcomes and surgical strategies in revision cervical arthroplasty following M6-C™ disc-related osteolysis.Eur Spine J. 2025 Aug;34(8):3365-3375. doi: 10.1007/s00586-025-08926-6. Epub 2025 May 28. Eur Spine J. 2025. PMID: 40434584
References
-
- Vos T, Allen C, Arora M, et al. . Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1545–1602. 10.1016/S0140-6736(16)31678-6 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources