

Spontaneous breathing promotes lung injury in an experimental model of alveolar collapse
- PMID: 35879511
- PMCID: PMC9310356
- DOI: 10.1038/s41598-022-16446-2
Spontaneous breathing promotes lung injury in an experimental model of alveolar collapse
Abstract
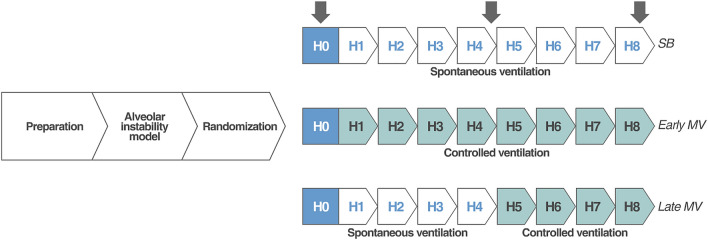
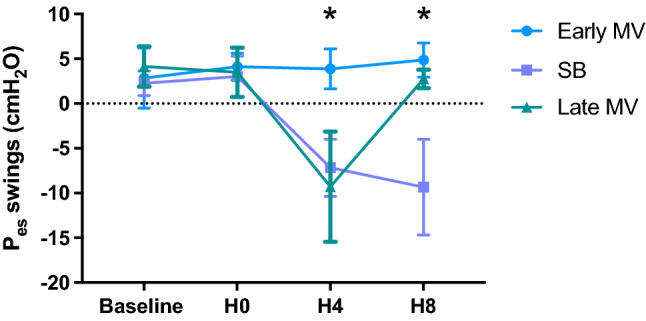
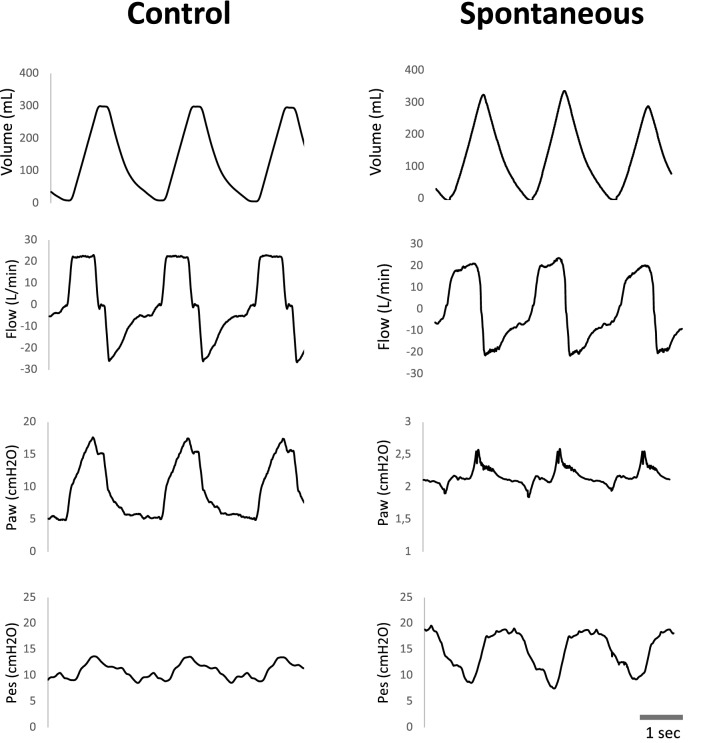
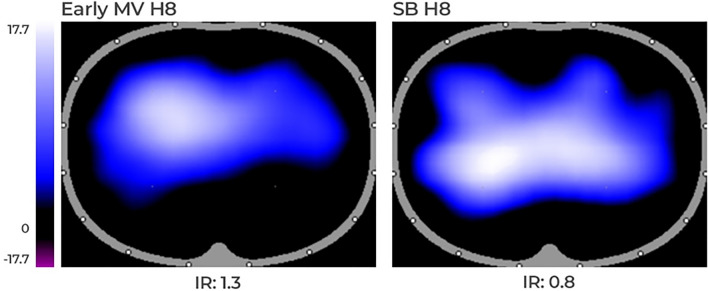
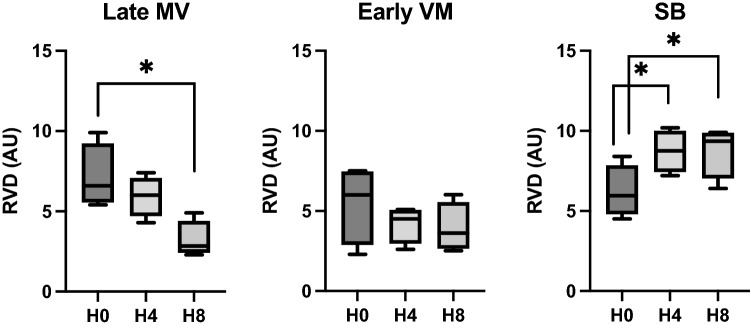
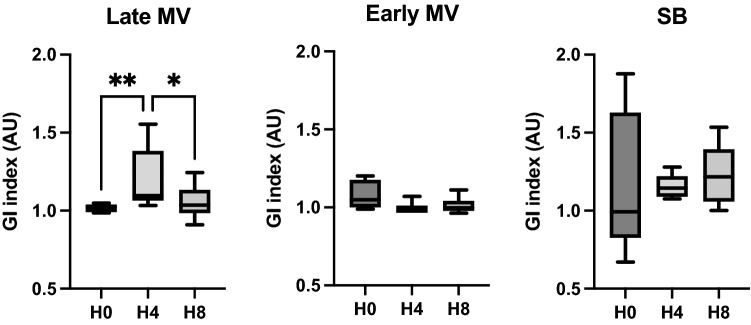
Vigorous spontaneous breathing has emerged as a promotor of lung damage in acute lung injury, an entity known as "patient self-inflicted lung injury". Mechanical ventilation may prevent this second injury by decreasing intrathoracic pressure swings and improving regional air distribution. Therefore, we aimed to determine the effects of spontaneous breathing during the early stage of acute respiratory failure on lung injury and determine whether early and late controlled mechanical ventilation may avoid or revert these harmful effects. A model of partial surfactant depletion and lung collapse was induced in eighteen intubated pigs of 32 ±4 kg. Then, animals were randomized to (1) SB-group: spontaneous breathing with very low levels of pressure support for the whole experiment (eight hours), (2) Early MV-group: controlled mechanical ventilation for eight hours, or (3) Late MV-group: first half of the experiment on spontaneous breathing (four hours) and the second half on controlled mechanical ventilation (four hours). Respiratory, hemodynamic, and electric impedance tomography data were collected. After the protocol, animals were euthanized, and lungs were extracted for histologic tissue analysis and cytokines quantification. SB-group presented larger esophageal pressure swings, progressive hypoxemia, lung injury, and more dorsal and inhomogeneous ventilation compared to the early MV-group. In the late MV-group switch to controlled mechanical ventilation improved the lung inhomogeneity and esophageal pressure swings but failed to prevent hypoxemia and lung injury. In a lung collapse model, spontaneous breathing is associated to large esophageal pressure swings and lung inhomogeneity, resulting in progressive hypoxemia and lung injury. Mechanical ventilation prevents these mechanisms of patient self-inflicted lung injury if applied early, before spontaneous breathing occurs, but not when applied late.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
