

Novel balloon compression-assisted endoscopic injection sclerotherapy and endoscopic variceal ligation in the treatment of esophageal varices: a prospective randomized study
- PMID: 35879573
- PMCID: PMC9485182
- DOI: 10.1007/s00464-022-09412-6
Novel balloon compression-assisted endoscopic injection sclerotherapy and endoscopic variceal ligation in the treatment of esophageal varices: a prospective randomized study
Abstract
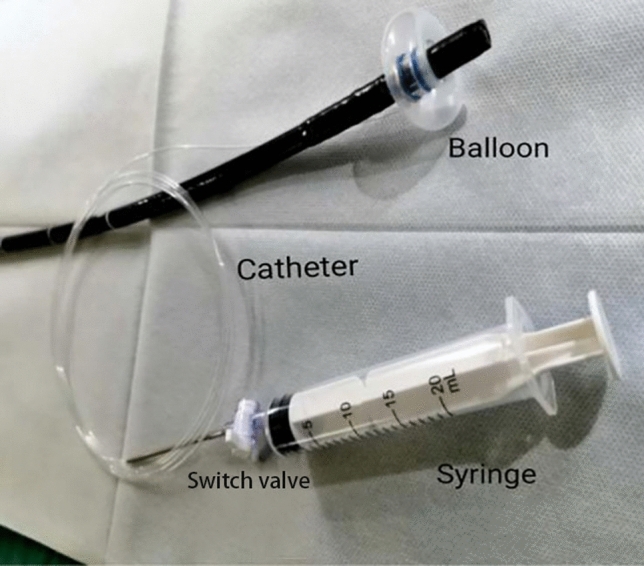
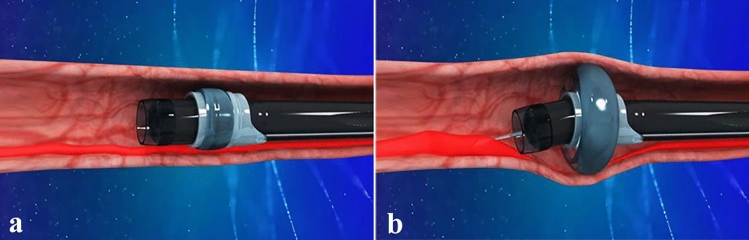
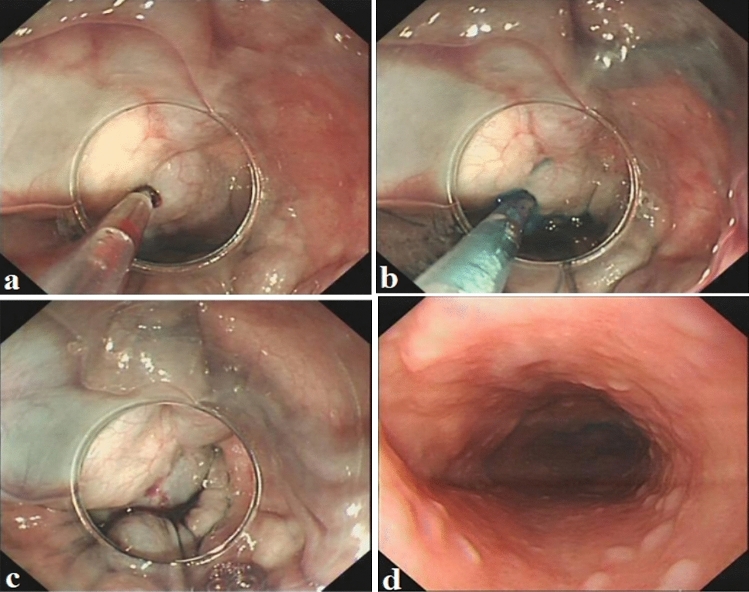
Background: Herein, our group designed a novel technology, termed balloon compression-assisted endoscopic injection sclerotherapy (bc-EIS), which was applied to improve the efficiency of eradicating esophageal varices (EVs). The present study aimed to compare the rate of eradication and efficacy between bc-EIS and endoscopic variceal ligation (EVL) in the management of EVs.
Methods: Ninety-five patients with esophageal variceal bleeding (EVB) were randomly assigned to receive bc-EIS or ligation alone. Additional treatment sessions were held 1 month later and then at 3-month intervals until eradication of the varices was achieved. Endoscopic follow-up examinations were carried out at 6-month intervals in the absence of recurrence or immediately if there was any recurrent bleeding.
Results: The mean physical injection points per session were 2.89 ± 0.79, and the mean volume of lauromacrogol used per session was 17.74 ± 7.09 ml in the bc-EIS group. The mean band per session was 6.13 ± 0.86. The rate of eradication after one to three rounds of bc-EIS was obviously higher than that of the EVL group (89.36%, 97.87%, and 100% vs. 37.5%, 43.75%, and 47.92%, respectively). Retrosternal pain or discomfort in the bc-EIS group was slightly lower than that in the EVL group (23.4%, 11/47 vs. 31.25%, 15/48). Two and five patients showed mild abdominal bloating and distension between the bc-EIS and EVL groups, respectively (2/47, 4.26% vs. 5/48, 10.42% P > 0.05). Nausea and vomiting were reported in one patient (1/47, 2.13%) in the bc-EIS group and three patients (3/48, 6.25%) in the EVL group. However, there were no statistically significant differences between the two groups (P > 0.05). No fatal or severe complications, such as esophageal perforation, esophageal stricture or ectopic embolism, were observed.
Conclusion: The bc-EIS method was effective in eradicating EVs and was accompanied by fewer complications.
Keywords: Balloon compression-assisted endoscopic injection sclerotherapy; Cirrhosis; Endoscopic injection sclerotherapy; Endoscopic variceal ligation; Esophageal variceal bleeding; Esophageal varices.
© 2022. The Author(s).
Conflict of interest statement
Qianqian Zhang, Jing Jin, Fumin Zhang, Yi Xiang, Wenyue Wu, Zexue Wang, and Derun Kong have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Krige J, Jonas E, Kotze U, Kloppers C, Gandhi K, Allam H, Bernon M, Burmeister S, Setshedi M. Defining the advantages and exposing the limitations of endoscopic variceal ligation in controlling acute bleeding and achieving complete variceal eradication. World J Gastrointest Endosc. 2020;12:365–377. doi: 10.4253/wjge.v12.i10.365. - DOI - PMC - PubMed
-
- Marusic M, Klemencic A, Troskot PR, Hauser G. Gastroesophageal variceal bleeding—an overview of current treatment options. Acta Gastroenterol Belg. 2018;81:305–317. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
