

What Is New in the Anti- Pseudomonas aeruginosa Clinical Development Pipeline Since the 2017 WHO Alert?
- PMID: 35880080
- PMCID: PMC9308001
- DOI: 10.3389/fcimb.2022.909731
What Is New in the Anti- Pseudomonas aeruginosa Clinical Development Pipeline Since the 2017 WHO Alert?
Abstract
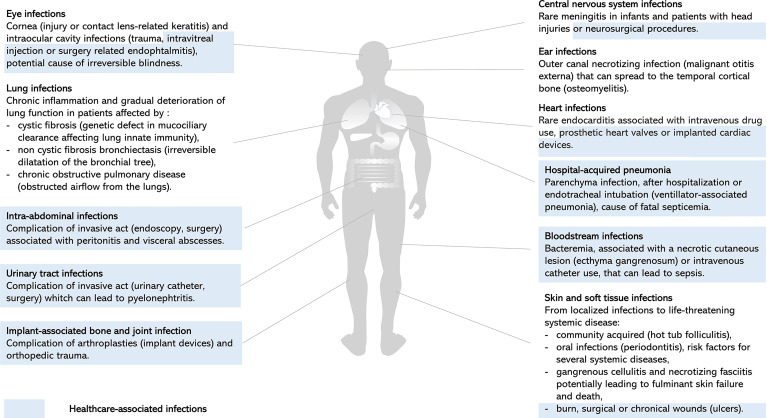
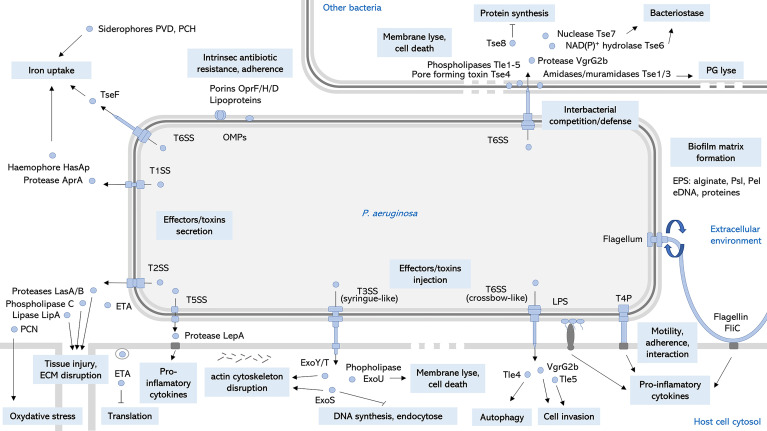
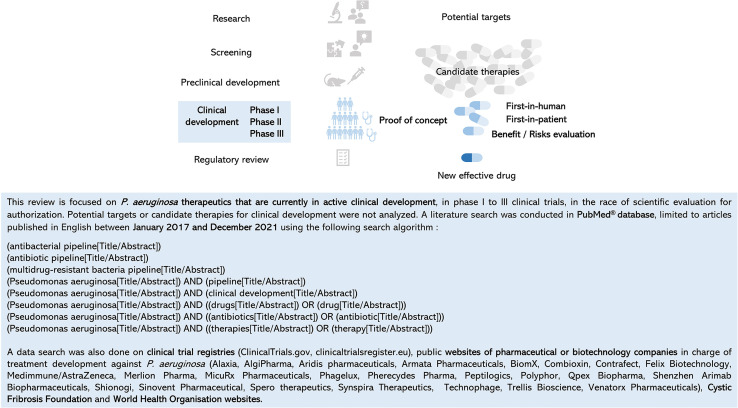
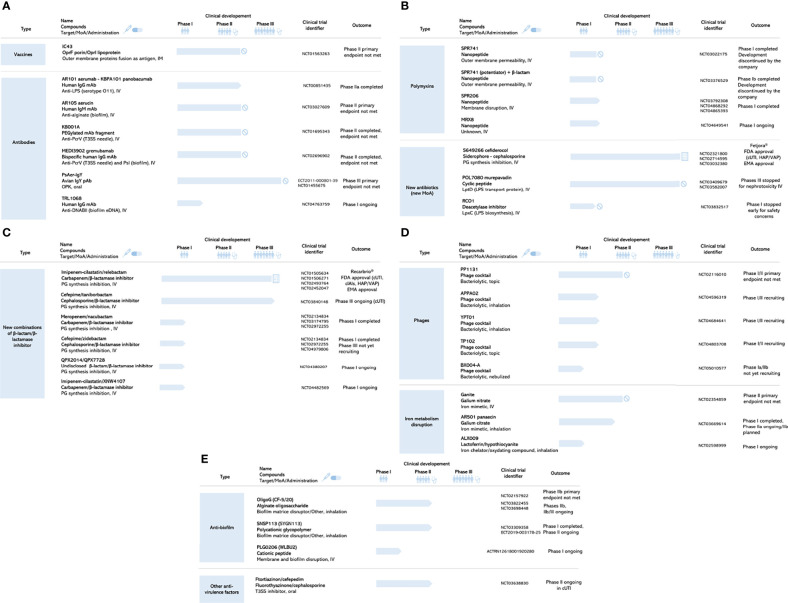
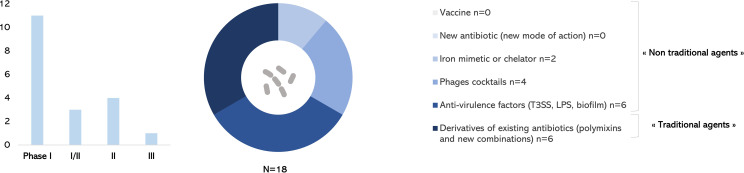
The spread of antibiotic-resistant bacteria poses a substantial threat to morbidity and mortality worldwide. Carbapenem-resistant Pseudomonas aeruginosa (CRPA) are considered "critical-priority" bacteria by the World Health Organization (WHO) since 2017 taking into account criteria such as patient mortality, global burden disease, and worldwide trend of multi-drug resistance (MDR). Indeed P. aeruginosa can be particularly difficult to eliminate from patients due to its combinatory antibiotic resistance, multifactorial virulence, and ability to over-adapt in a dynamic way. Research is active, but the course to a validated efficacy of a new treatment is still long and uncertain. What is new in the anti-P. aeruginosa clinical development pipeline since the 2017 WHO alert? This review focuses on new solutions for P. aeruginosa infections that are in active clinical development, i.e., currently being tested in humans and may be approved for patients in the coming years. Among 18 drugs of interest in December 2021 anti-P. aeruginosa development pipeline described here, only one new combination of β-lactam/β-lactamase inhibitor is in phase III trial. Derivatives of existing antibiotics considered as "traditional agents" are over-represented. Diverse "non-traditional agents" including bacteriophages, iron mimetic/chelator, and anti-virulence factors are significantly represented but unfortunately still in early clinical stages. Despite decade of efforts, there is no vaccine currently in clinical development to prevent P. aeruginosa infections. Studying pipeline anti-P. aeruginosa since 2017 up to now shows how to provide a new treatment for patients can be a difficult task. Given the process duration, the clinical pipeline remains unsatisfactory leading best case to the approval of new antibacterial drugs that treat CRPA in several years. Beyond investment needed to build a robust pipeline, the Community needs to reinvent medicine with new strategies of development to avoid the disaster. Among "non-traditional agents", anti-virulence strategy may have the potential through novel and non-killing modes of action to reduce the selective pressure responsible of MDR.
Keywords: Pseudomonas aeruginosa; anti-virulence strategy; antibiotics; development pipeline; immunotherapy; multi-drug resistance; phage therapy; vaccine.
Copyright © 2022 Reig, Le Gouellec and Bleves.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. SR is currently working in the Medical Department of Novartis Gene Therapies France SAS as Senior Medical Science Manager. SR is a PhD student independently of his professional position and on a totally different therapeutic area.
Figures
Similar articles
-
The Therapeutic Pipeline for Pseudomonas aeruginosa Infections.ACS Infect Dis. 2018 Jul 13;4(7):1041-1047. doi: 10.1021/acsinfecdis.8b00112. Epub 2018 May 17. ACS Infect Dis. 2018. PMID: 29771109 Review.
-
Relationship between antibiotic resistance, biofilm formation, genes coding virulence factors and source of origin of Pseudomonas aeruginosa clinical strains.Ann Agric Environ Med. 2021 Jun 14;28(2):306-313. doi: 10.26444/aaem/122682. Epub 2020 Jun 4. Ann Agric Environ Med. 2021. PMID: 34184515
-
Molecular characterizations of antibiotic resistance, biofilm formation, and virulence determinants of Pseudomonas aeruginosa isolated from burn wound infection.J Clin Lab Anal. 2023 Apr;37(4):e24850. doi: 10.1002/jcla.24850. Epub 2023 Feb 17. J Clin Lab Anal. 2023. PMID: 36808649 Free PMC article.
-
Risk factors for mortality in patients with bloodstream infections caused by carbapenem-resistant Pseudomonas aeruginosa: clinical impact of bacterial virulence and strains on outcome.Diagn Microbiol Infect Dis. 2014 Oct;80(2):130-5. doi: 10.1016/j.diagmicrobio.2014.07.003. Epub 2014 Jul 17. Diagn Microbiol Infect Dis. 2014. PMID: 25112900
-
Pseudomonas aeruginosa chromosomal beta-lactamase in patients with cystic fibrosis and chronic lung infection. Mechanism of antibiotic resistance and target of the humoral immune response.APMIS Suppl. 2003;(116):1-47. APMIS Suppl. 2003. PMID: 14692154 Review.
Cited by
-
Antimicrobial Resistance and Genetic Diversity of Pseudomonas aeruginosa Strains Isolated from Equine and Other Veterinary Samples.Pathogens. 2022 Dec 30;12(1):64. doi: 10.3390/pathogens12010064. Pathogens. 2022. PMID: 36678412 Free PMC article.
-
Transcriptional Regulators Controlling Virulence in Pseudomonas aeruginosa.Int J Mol Sci. 2023 Jul 25;24(15):11895. doi: 10.3390/ijms241511895. Int J Mol Sci. 2023. PMID: 37569271 Free PMC article. Review.
-
Making a chink in their armor: Current and next-generation antimicrobial strategies against the bacterial cell envelope.Adv Microb Physiol. 2023;83:221-307. doi: 10.1016/bs.ampbs.2023.05.003. Epub 2023 Jun 27. Adv Microb Physiol. 2023. PMID: 37507160 Free PMC article.
-
Evolution of two metabolic genes involved in nucleotide and amino acid metabolism in Pseudomonas aeruginosa.PLoS One. 2024 Dec 17;19(12):e0315931. doi: 10.1371/journal.pone.0315931. eCollection 2024. PLoS One. 2024. PMID: 39689084 Free PMC article.
-
Resistance in Pseudomonas aeruginosa: A Narrative Review of Antibiogram Interpretation and Emerging Treatments.Antibiotics (Basel). 2023 Nov 12;12(11):1621. doi: 10.3390/antibiotics12111621. Antibiotics (Basel). 2023. PMID: 37998823 Free PMC article. Review.
References
-
- Adlbrecht C., Wurm R., Depuydt P., Spapen H., Lorente J. A., Staudinger T., et al. . (2020). Efficacy, Immunogenicity, and Safety of IC43 Recombinant Pseudomonas Aeruginosa Vaccine in Mechanically Ventilated Intensive Care Patients-a Randomized Clinical Trial. Crit. Care 24 (1), 74. doi: 10.1186/s13054-020-2792-z - DOI - PMC - PubMed
-
- Alhazmi A. (2015). Pseudomonas Aeruginosa – Pathogenesis and Pathogenic Mechanisms. Int. J. Biology; 7, 44–67. doi: 10.5539/ijb.v7n2p44 - DOI
-
- Ali S. O., Yu X. Q., Robbie G. J., Wu Y., Shoemaker K., Yu L., et al. . (2019). Phase 1 Study of MEDI3902, an Investigational Anti-Pseudomonas Aeruginosa PcrV and Psl Bispecific Human Monoclonal Antibody, in Healthy Adults. Clin. Microbiol. Infect. 25 (5), 629.e1–629.e6. doi: 10.1016/j.cmi.2018.08.004 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources