

Cohort Comparison of Radiographic Correction and Complications Between Minimal Invasive and Open Lapidus Procedures for Hallux Valgus
- PMID: 35880322
- PMCID: PMC9527364
- DOI: 10.1177/10711007221112088
Cohort Comparison of Radiographic Correction and Complications Between Minimal Invasive and Open Lapidus Procedures for Hallux Valgus
Abstract
Background: The Lapidus procedure corrects hallux valgus first ray deformity. First tarsometatarsal (TMT) fusion in patients with hallux valgus deformity using minimally invasive surgery (MIS) is a new technique, but comparative outcomes between MIS and open techniques have not been reported. This study compares the early radiographic results and complications of the MIS with the open procedure in a single-surgeon practice.
Methods: 47 MIS patients were compared with 44 open patients. Radiographic measures compared preoperatively and postoperatively were the intermetatarsal angle (IMA), hallux valgus angle (HVA), foot width (FW), distal metatarsal articular angle (DMAA), sesamoid station (SS), metatarsus adductus angle (MAA), first metatarsal to second metatarsal length, and elevation of the first metatarsal. Early complications were recorded, as well as repeat surgeries.
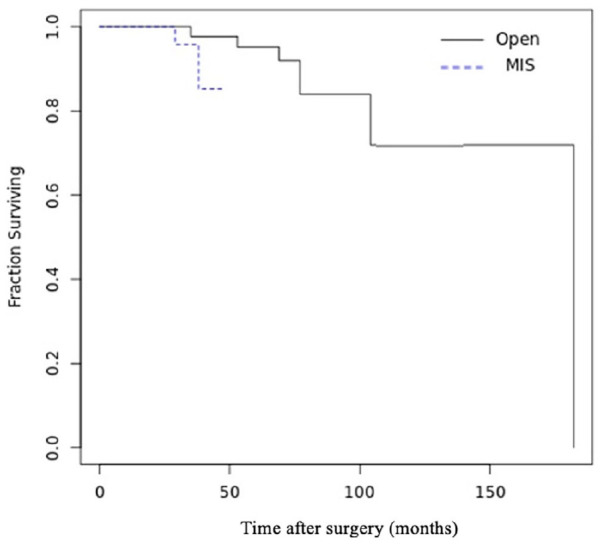
Results: The mean follow-up was 82 (range, 31-182) months for the open group and 29 (range, 14-47) months for the MIS group. In both techniques, postoperative measures (IMA, HVA, DMAA, FW, and sesamoid station) were significantly improved from preoperative measures. When comparing postoperative measures between both groups, the IMA was significantly lower in the open group (4.8 ± 3.6 degrees vs 6.4 ± 3.2 degrees, P < .05). Differential between pre- and postoperative measures for both techniques were compared, and the open group was associated with more correction than the MIS group for IMA (12.4 ± 5.3 degrees vs 9.4 ± 4.4 degrees, P = .004) and HVA (25.5 ± 8.3 degrees vs 20 ± 9.9 degrees, P = .005). Wound complication and nonunion rates trended higher in the open group (4 vs 0) (P = .051).
Conclusion: Both techniques resulted in good to excellent correction. However, the open technique was associated with lower postoperative IMA values and more correction power for IMA and HVA, than the MIS.
Keywords: Lapidus; arthroscopy; first tarsometatarsal fusion; hallux valgus; minimally invasive surgery.
Conflict of interest statement
Figures



Similar articles
-
Utilization of the Modified Lapidus Procedure for Correction of Moderate to Severe Hallux Valgus Deformity With Increased Distal Metatarsal Articular Angle.Foot Ankle Spec. 2024 Aug;17(4):352-357. doi: 10.1177/19386400221093859. Epub 2022 May 24. Foot Ankle Spec. 2024. PMID: 35608239
-
Radiographic Evaluation of Intermetatarsal Angle Correction Following First MTP Joint Arthrodesis for Severe Hallux Valgus.Foot Ankle Int. 2016 Nov;37(11):1183-1186. doi: 10.1177/1071100716656442. Epub 2016 Jul 11. Foot Ankle Int. 2016. PMID: 27405308
-
A prospective study to compare the operative outcomes of minimally invasive proximal and distal chevron metatarsal osteotomy for moderate-to-severe hallux valgus deformity.Int Orthop. 2021 Nov;45(11):2933-2943. doi: 10.1007/s00264-021-05106-1. Epub 2021 Jul 17. Int Orthop. 2021. PMID: 34272980
-
Modified Lindgren-Turan Osteotomy for Hallux Valgus Deformity - a Review of 60 Cases.Acta Chir Orthop Traumatol Cech. 2018;85(5):325-330. Acta Chir Orthop Traumatol Cech. 2018. PMID: 30383528 Review. English.
-
Minimally Invasive vs. Open Surgery for Hallux Valgus: A Meta-Analysis.Front Surg. 2022 Mar 21;9:843410. doi: 10.3389/fsurg.2022.843410. eCollection 2022. Front Surg. 2022. PMID: 35388365 Free PMC article.
Cited by
-
Comparison of Minimally Invasive Chevron Akin and Open Lapidus Surgery in Older Patients at a Minimum 1-Year Follow-Up.Foot Ankle Orthop. 2024 Jul 30;9(3):24730114241266843. doi: 10.1177/24730114241266843. eCollection 2024 Jul. Foot Ankle Orthop. 2024. PMID: 39091403 Free PMC article.
-
Minimally Invasive Forefoot Surgeries Using the Shannon Burr: A Comprehensive Review.Diagnostics (Basel). 2024 Aug 29;14(17):1896. doi: 10.3390/diagnostics14171896. Diagnostics (Basel). 2024. PMID: 39272681 Free PMC article. Review.
-
Clinical and radiological outcome of surgical hallux valgus correction: open versus minimally invasive.Eur J Orthop Surg Traumatol. 2024 Aug;34(6):3329-3337. doi: 10.1007/s00590-024-04074-7. Epub 2024 Aug 20. Eur J Orthop Surg Traumatol. 2024. PMID: 39162733 Free PMC article.
-
A Multi-Dimensional Systematic Review of Minimally Invasive Bunion Surgery (MIBS).J Clin Med. 2025 Apr 17;14(8):2757. doi: 10.3390/jcm14082757. J Clin Med. 2025. PMID: 40283587 Free PMC article. Review.
References
-
- de Las Heras-Romero J, Lledó-Alvarez AM, Andrés-Grau J, Picazo-Marín F, Moreno-Sánchez JF, Hernández-Torralba M. A new minimally extended distal Chevron osteotomy (MEDCO) with percutaneous soft tissue release (PSTR) for treatment of moderate hallux valgus. Foot (Edinb). 2019;40: 27-33. doi:10.1016/j.foot.2019.04.001 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
