

Vericiguat and NT-proBNP in patients with heart failure with reduced ejection fraction: analyses from the VICTORIA trial
- PMID: 35880474
- PMCID: PMC9773767
- DOI: 10.1002/ehf2.14050
Vericiguat and NT-proBNP in patients with heart failure with reduced ejection fraction: analyses from the VICTORIA trial
Abstract
Aims: Treatment response to vericiguat, based on baseline N-terminal pro-brain natriuretic peptide (NT-proBNP) subgroups specified in the protocol, was evaluated in the heart failure (HF) VICTORIA trial population by post hoc analysis of combined lower three quartiles [Q1-Q3] vs. the upper quartile [Q4].
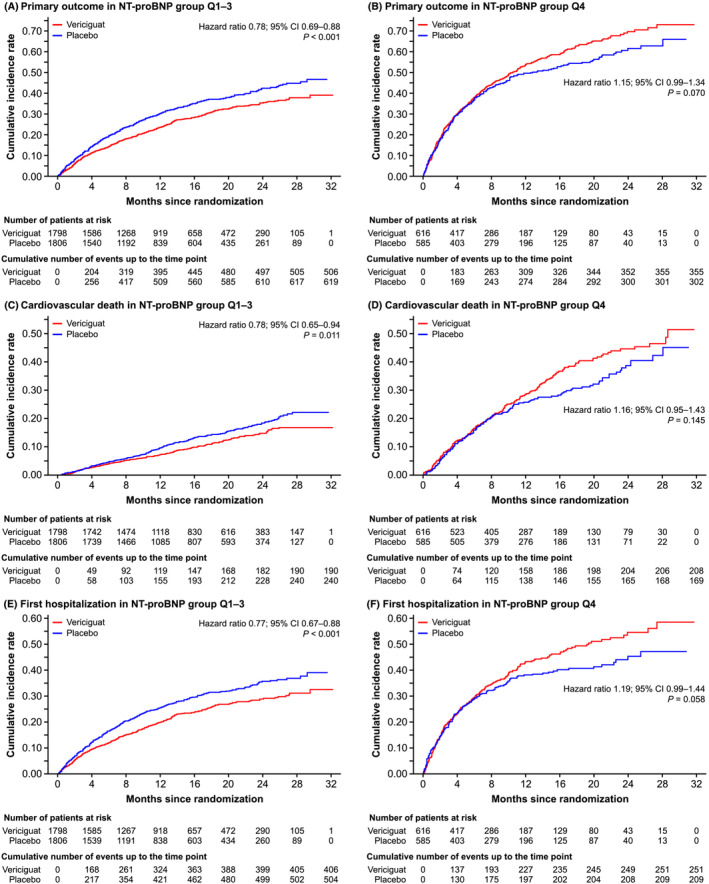
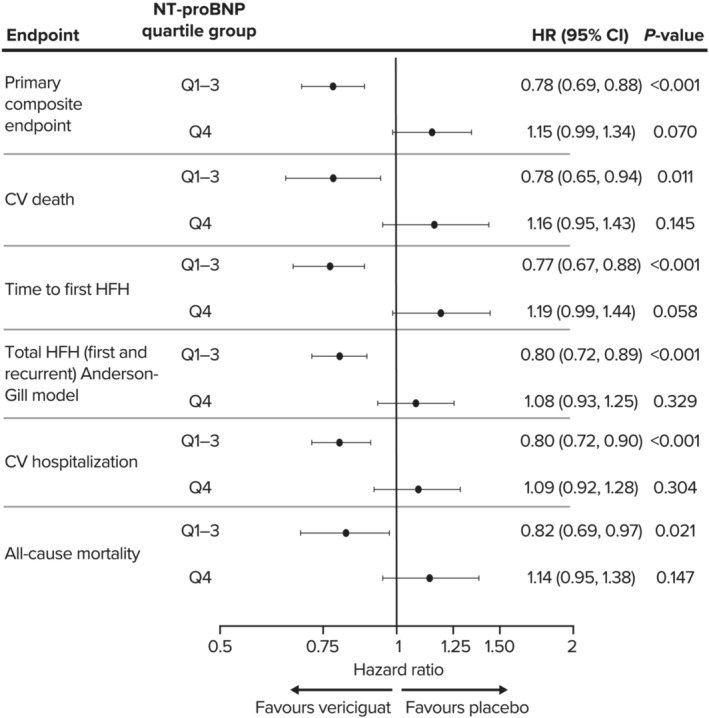
Methods and results: VICTORIA participants with available baseline NT-proBNP levels (n = 4805; 95.1% of total) were included. Compared with patients in Q1-Q3 (NT-proBNP: Q1, ≤1556 pg/mL; Q2, >1556-2816 pg/mL; and Q3, >2816-5314 pg/mL), patients in Q4 (NT-proBNP: >5314 pg/mL) were older (69.2 ± 12.0 vs. 66.6 ± 12.1 years), had lower mean ejection fraction (27.2 ± 8.3% vs. 29.5 ± 8.2%; P < 0.0001), and were more likely to be in New York Heart Association (NYHA) Class III (51.8 vs. 35.6%) or IV (2.4 vs. 1.0%). Compared with Q1-Q3, patients in Q4 had higher mean Meta-Analysis Global Group in Chronic Heart Failure risk score (27.3 ± 6.6 vs. 23.5 ± 6.4; P < 0.0001), had lower mean estimated glomerular filtration rate (eGFR; 51.5 ± 25.5 vs. 65.0 ± 26.8 mL/min/1.73 m2 ; P < 0.0001) and haemoglobin (12.8 ± 2.0 vs. 13.6 ± 1.9 g/dL; P < 0.0001), and more had atrial fibrillation (48.7% vs. 43.1%; P = 0.0007) and were randomized while hospitalized for HF (14.8 vs. 9.9%; P < 0.0001). Target dose was achieved in 72.3 and 63.7% of patients in Q1-Q3 and Q4, respectively (P < 0.0001). Primary outcome (composite of time to cardiovascular death or first HF hospitalization) rates were 24.5 and 31.7 per 100 patient-years for vericiguat and placebo in Q1-Q3 [hazard ratio (HR) 0.78; 95% confidence interval (CI) 0.69-0.88, P < 0.001] and 73.6 and 63.6 in Q4 (HR 1.15; 95% CI 0.99-1.34, P = 0.070). Serious adverse events were more frequent in NT-proBNP Q4 (total population) compared with Q1-Q3 (38.3 vs. 32.3%; P = 0.0001), driven mainly by the placebo group. Adverse events leading to death were more frequent in Q4 than Q1-Q3 (5.8 vs. 2.4%; P < 0.0001).
Conclusions: Plasma NT-proBNP may help identify patients with worsening HF with reduced ejection fraction, in whom the beneficial effects of vericiguat may be highest. Patients with highest NT-proBNP values are probably too far advanced, suffering more co-morbidities, or still clinically unstable after decompensation to derive benefit from vericiguat.
Trial registration: ClinicalTrials.gov NCT02861534.
Keywords: Heart failure; Heart failure with reduced ejection fraction; NT-proBNP.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
RN, CF, VMV, and LR are employees of Bayer AG and may own stock in the company. ACS has received honoraria from Bayer AG and Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA (MSD), during the conduct of the study; and personal fees from Novartis, Abbott, Sanofi, Vifor, Astra Zeneca, Servier, Leo Pharma, and Boehringer Ingelheim, outside the submitted work. JLS has received research grants from MSD, Angem, Pfizer, and Bayer AG; honoraria from Menarini; support for attending meetings from Pfizer; and support for participation on advisory boards from Bayer AG. MS has received consulting fees from Bayer AG and MSD. PP has received consulting fees from Boehringer Ingelheim, AstraZeneca, Vifor Pharma, Amgen, Servier, Novartis, Bayer, MSD, Pfizer, Cibiem, Impulse Dynamics, Renal Guard Solutions, and BMS. PP has also received honoraria from Boehringer Ingelheim, AstraZeneca, Vifor Pharma, Amgen, Servier, Novartis, Berlin Chemie, Bayer, Pfizer, Impulse Dynamics, Renal Guard Solutions, BMS, and Abbott Vascular for lectures, presentations, speakers' bureaus, manuscript writing, or educational events. BP has received research funds from Bayer Healthcare, Servier, and AstraZeneca, as well as speakers honoraria/committee membership fees from Novartis, Bayer Healthcare, Daiichi‐Sankyo, MSD, Stealth Peptides, AstraZeneca, Sanofi, Vifor, and Servier.
Figures
References
-
- Gaggin HK, Truong QA, Rehman SU, Mohammed AA, Bhardwaj A, Parks KA, Sullivan DA, Chen‐Tournoux A, Moore SA, Richards AM, Troughton RW, Lainchbury JG, Weiner RB, Baggish AL, Semigran MJ, Januzzi JL Jr. Characterization and prediction of natriuretic peptide “nonresponse” during heart failure management: Results from the ProBNP outpatient tailored chronic heart failure (PROTECT) and the NT‐proBNP‐assisted treatment to lessen serial cardiac readmissions and death (BATTLESCARRED) study. Congest Heart Fail. 2013; 19: 135–142. - PubMed
-
- Armstrong PW, Pieske B, Anstrom KJ, Ezekowitz J, Hernandez AF, Butler J, Lam CSP, Ponikowski P, Voors AA, Jia G, McNulty SE, Patel MJ, Roessig L, Koglin J, O'Connor CM. Vericiguat in patients with heart failure and reduced ejection fraction. N Engl J Med. 2020; 382: 1883–1893. - PubMed
-
- Ezekowitz JA, O'Connor CM, Troughton RW, Alemayehu WG, Westerhout CM, Voors AA, Butler J, Lam CSP, Ponikowski P, Emdin M, Patel MJ, Pieske B, Roessig L, Hernandez AF, Armstrong PW. N‐terminal pro‐B‐type natriuretic peptide and clinical outcomes: Vericiguat heart failure with reduced ejection fraction study. JACC Heart Fail. 2020; 8: 931–939. - PubMed
-
- Food and Drug Administration . Verquvo™ (vericiguat) tablets. Highlights of prescribing information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/214377s000lbl.pdf. Accessed Feb 08, 2021.
-
- Armstrong PW, Roessig L, Patel MJ, Anstrom KJ, Butler J, Voors AA, Lam CSP, Ponikowski P, Temple T, Pieske B, Ezekowitz J, Hernandez AF, Koglin J, O'Connor CM. A multicenter, randomized, double‐blind, placebo‐controlled trial of the efficacy and safety of the oral soluble guanylate cyclase stimulator: The VICTORIA trial. JACC Heart Fail. 2018; 6: 96–104. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
