

Surgical Considerations for Tumor Tissue Procurement to Obtain Tumor-Infiltrating Lymphocytes for Adoptive Cell Therapy
- PMID: 35880938
- PMCID: PMC9335895
- DOI: 10.1097/PPO.0000000000000608
Surgical Considerations for Tumor Tissue Procurement to Obtain Tumor-Infiltrating Lymphocytes for Adoptive Cell Therapy
Abstract
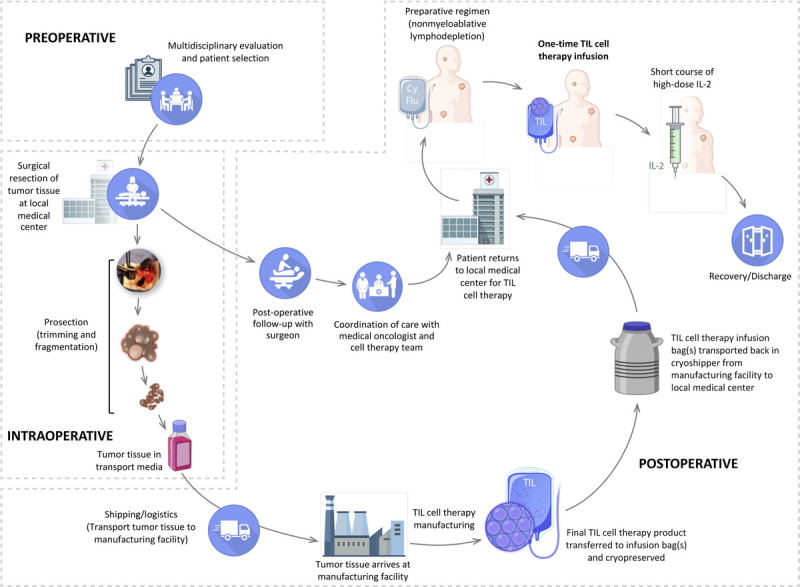
Adoptive cell therapy with tumor-infiltrating lymphocytes (TILs), an investigational cellular therapy, has demonstrated antitumor efficacy in patients with advanced solid tumors, including melanoma. Tumor-infiltrating lymphocyte cell therapy involves surgical resection of a patient's tumor, ex vivo TIL expansion under conditions that overcome immunosuppressive responses elicited by the tumor and the tumor microenvironment, administration of a lymphodepleting regimen, and infusion of the final TIL cell therapy product back into the patient followed by interleukin 2 administration to support T-cell activity. The surgeon plays a central role in patient identification and tumor selection-steps that are critical for successful outcomes of TIL cell therapy. Commercialization of TIL cell therapy and its broader access to patients will require education and collaboration among surgeons, oncologists, and cellular therapists. This review highlights the unique role that surgeons will play in the implementation of TIL cell therapy and serves as a contemporary report of best practices for patient selection and tumor resection methods.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Conflicts of Interest and Source of Funding: The authors have disclosed that they have no significant relationships with, or financial interest in, any commercial companies pertaining to this article. Medical writing support, funded by Iovance Biotherapeutics (with specific direction and input from authors), was provided by Swati Ghatpande, PhD, and Jerylin Gan, PhD, of Second City Science (Vaniam Group LLC).
Figures
Similar articles
-
Expert consensus guidelines on management and best practices for tumor-infiltrating lymphocyte cell therapy.J Immunother Cancer. 2024 Feb 29;12(2):e008735. doi: 10.1136/jitc-2023-008735. J Immunother Cancer. 2024. PMID: 38423748 Free PMC article. Review.
-
Tumor-infiltrating lymphocytes for adoptive cell therapy: recent advances, challenges, and future directions.Expert Opin Biol Ther. 2022 May;22(5):627-641. doi: 10.1080/14712598.2022.2064711. Epub 2022 Apr 20. Expert Opin Biol Ther. 2022. PMID: 35414331 Review.
-
Adherent cell depletion promotes the expansion of renal cell carcinoma infiltrating T cells with optimal characteristics for adoptive transfer.J Immunother Cancer. 2020 Oct;8(2):e000706. doi: 10.1136/jitc-2020-000706. J Immunother Cancer. 2020. PMID: 33037114 Free PMC article.
-
Achievements and challenges of adoptive T cell therapy with tumor-infiltrating or blood-derived lymphocytes for metastatic melanoma: what is needed to achieve standard of care?Cancer Immunol Immunother. 2014 Oct;63(10):1081-91. doi: 10.1007/s00262-014-1580-5. Epub 2014 Aug 7. Cancer Immunol Immunother. 2014. PMID: 25099366 Free PMC article. Review.
-
Tumor-Infiltrating Lymphocyte Therapy in Melanoma: Facts to the Future.Clin Cancer Res. 2023 May 15;29(10):1835-1854. doi: 10.1158/1078-0432.CCR-22-1922. Clin Cancer Res. 2023. PMID: 36485001 Free PMC article. Review.
Cited by
-
TIL Therapy in Lung Cancer: Current Progress and Perspectives.Adv Sci (Weinh). 2024 Dec;11(46):e2409356. doi: 10.1002/advs.202409356. Epub 2024 Oct 18. Adv Sci (Weinh). 2024. PMID: 39422665 Free PMC article. Review.
-
Tumor-Infiltrating Lymphocyte Cell Therapy for the Treatment of Advanced Melanoma: From Patient Identification to Posttreatment Management.J Adv Pract Oncol. 2025 Mar 16:1-14. doi: 10.6004/jadpro.2025.16.7.8. Online ahead of print. J Adv Pract Oncol. 2025. PMID: 40224920 Free PMC article. Review.
-
Biomarkers for response to TIL therapy: a comprehensive review.J Immunother Cancer. 2024 Mar 13;12(3):e008640. doi: 10.1136/jitc-2023-008640. J Immunother Cancer. 2024. PMID: 38485186 Free PMC article. Review.
-
Tumour-infiltrating lymphocyte therapy landscape: prospects and challenges.BMJ Oncol. 2025 Aug 4;4(1):e000566. doi: 10.1136/bmjonc-2024-000566. eCollection 2025. BMJ Oncol. 2025. PMID: 40765841 Free PMC article. Review.
-
Expert consensus guidelines on management and best practices for tumor-infiltrating lymphocyte cell therapy.J Immunother Cancer. 2024 Feb 29;12(2):e008735. doi: 10.1136/jitc-2023-008735. J Immunother Cancer. 2024. PMID: 38423748 Free PMC article. Review.
References
-
- Maeurer MJ Gollin SM Martin D, et al. . Tumor escape from immune recognition: lethal recurrent melanoma in a patient associated with downregulation of the peptide transporter protein TAP-1 and loss of expression of the immunodominant MART-1/Melan-A antigen. J Clin Invest. 1996;98:1633–1641. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
