

Effect of High- vs Low-Dose Tranexamic Acid Infusion on Need for Red Blood Cell Transfusion and Adverse Events in Patients Undergoing Cardiac Surgery: The OPTIMAL Randomized Clinical Trial
- PMID: 35881121
- PMCID: PMC9327582
- DOI: 10.1001/jama.2022.10725
Effect of High- vs Low-Dose Tranexamic Acid Infusion on Need for Red Blood Cell Transfusion and Adverse Events in Patients Undergoing Cardiac Surgery: The OPTIMAL Randomized Clinical Trial
Erratum in
-
Contributor Name Misspelled.JAMA. 2022 Nov 8;328(18):1873. doi: 10.1001/jama.2022.19835. JAMA. 2022. PMID: 36346427 Free PMC article. No abstract available.
Abstract
Importance: Tranexamic acid is recommended for reducing blood loss and transfusion in cardiac surgery. However, it remains unknown whether a high dose of tranexamic acid provides better blood-sparing effect than a low dose without increasing the risk of thrombotic complications or seizures in cardiac surgery.
Objective: To compare the efficacy and adverse events of high-dose vs low-dose tranexamic acid in patients undergoing cardiac surgery with cardiopulmonary bypass.
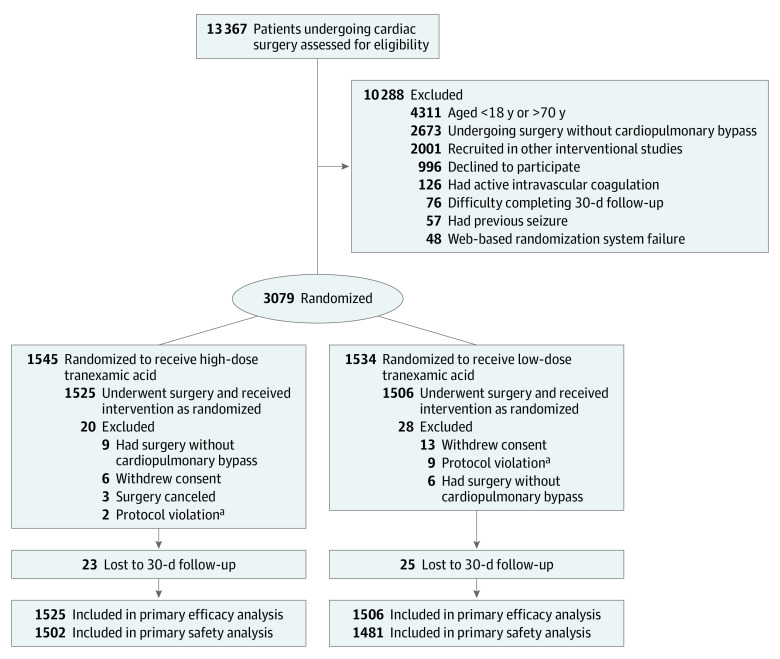
Design, setting, and participants: Multicenter, double-blind, randomized clinical trial among adult patients undergoing cardiac surgery with cardiopulmonary bypass. The study enrolled 3079 patients at 4 hospitals in China from December 26, 2018, to April 21, 2021; final follow-up was on May 21, 2021.
Interventions: Participants received either a high-dose tranexamic acid regimen comprising a 30-mg/kg bolus, a 16-mg/kg/h maintenance dose, and a 2-mg/kg prime (n = 1525) or a low-dose regimen comprising a 10-mg/kg bolus, a 2-mg/kg/h maintenance dose, and a 1-mg/kg prime (n = 1506).
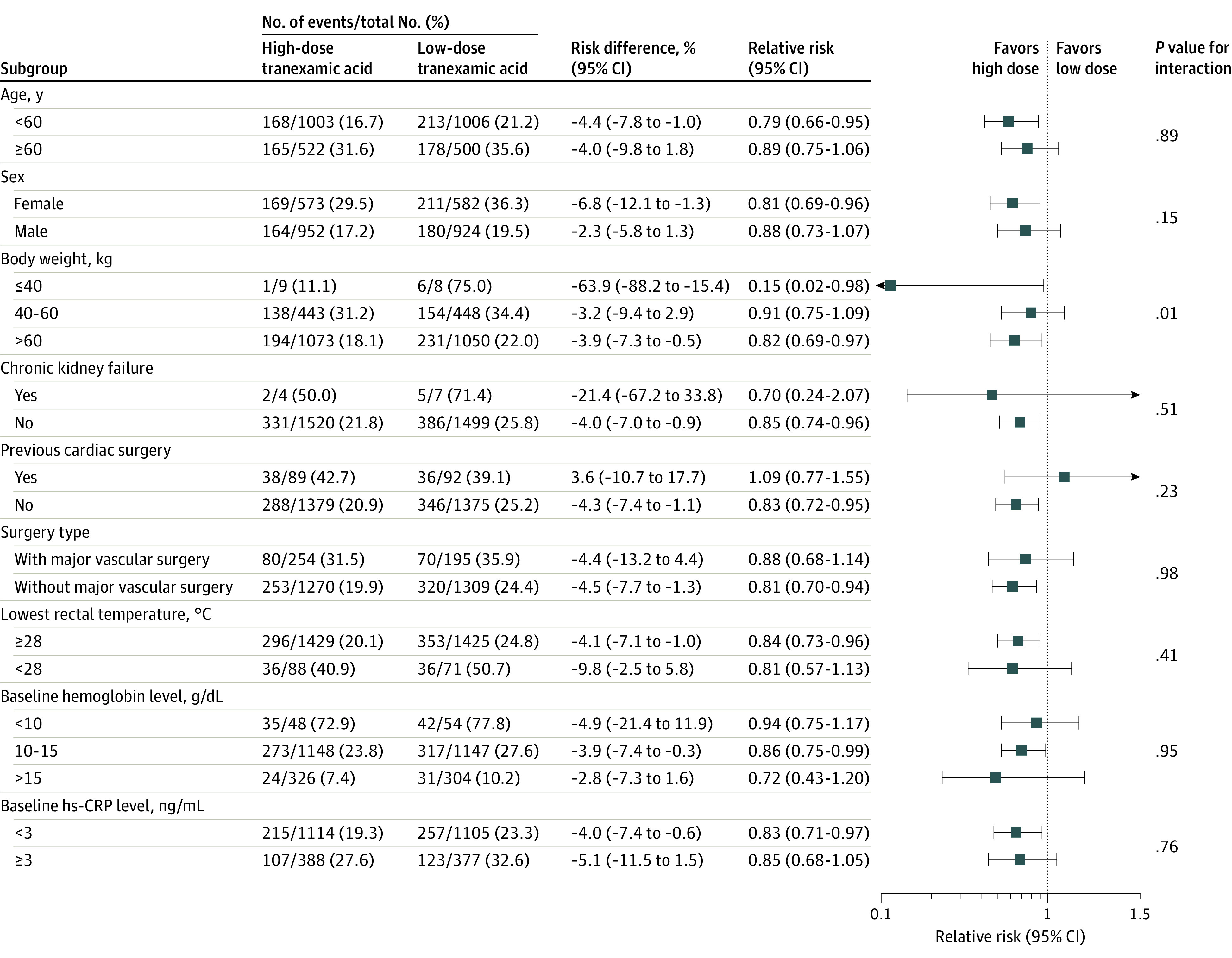
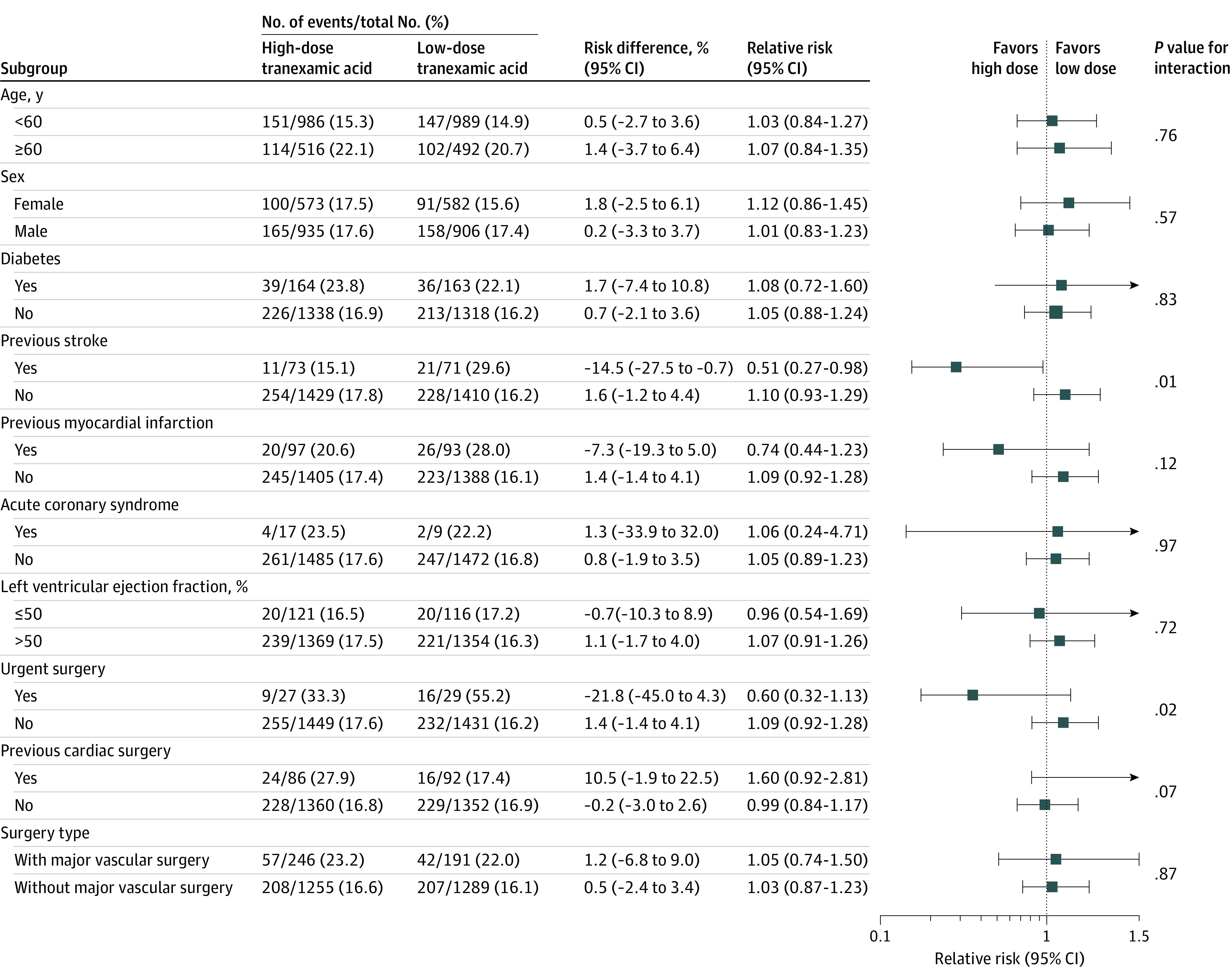
Main outcomes and measures: The primary efficacy end point was the rate of allogeneic red blood cell transfusion after start of operation (superiority hypothesis), and the primary safety end point was a composite of the 30-day postoperative rate of mortality, seizure, kidney dysfunction (stage 2 or 3 Kidney Disease: Improving Global Outcomes [KDIGO] criteria), and thrombotic events (myocardial infarction, ischemic stroke, deep vein thrombosis, and pulmonary embolism) (noninferiority hypothesis with a margin of 5%). There were 15 secondary end points, including the individual components of the primary safety end point.
Results: Among 3079 patients who were randomized to treatment groups (mean age, 52.8 years; 38.1% women), 3031 (98.4%) completed the trial. Allogeneic red blood cell transfusion occurred in 333 of 1525 patients (21.8%) in the high-dose group and 391 of 1506 patients (26.0%) in the low-dose group (risk difference [RD], -4.1% [1-sided 97.55% CI, -∞ to -1.1%]; relative risk, 0.84 [1-sided 97.55% CI, -∞ to 0.96; P = .004]). The composite of postoperative seizure, thrombotic events, kidney dysfunction, and death occurred in 265 patients in the high-dose group (17.6%) and 249 patients in the low-dose group (16.8%) (RD, 0.8%; 1-sided 97.55% CI, -∞ to 3.9%; P = .003 for noninferiority). Fourteen of the 15 prespecified secondary end points were not significantly different between groups, including seizure, which occurred in 15 patients (1.0%) in the high-dose group and 6 patients (0.4%) in the low-dose group (RD, 0.6%; 95% CI, -0.0% to 1.2%; P = .05).
Conclusions and relevance: Among patients who underwent cardiac surgery with cardiopulmonary bypass, high-dose compared with low-dose tranexamic acid infusion resulted in a modest statistically significant reduction in the proportion of patients who received allogeneic red blood cell transfusion and met criteria for noninferiority with respect to a composite primary safety end point consisting of 30-day mortality, seizure, kidney dysfunction, and thrombotic events.
Trial registration: ClinicalTrials.gov Identifier: NCT03782350.
Conflict of interest statement
Figures
Comment in
-
High- vs Low-Dose Tranexamic Acid Infusion and Need for Red Blood Cell Transfusion and Adverse Events in Cardiac Surgery.JAMA. 2023 Jan 3;329(1):97. doi: 10.1001/jama.2022.20277. JAMA. 2023. PMID: 36594951 No abstract available.
References
-
- Okamoto S, Okamoto U. Amino-methyl-cyclohexane-carboxylic acid: AMCHA: a new potent inhibitor of the fibrinolysis. Keio J Med. 1962;11(3):105-115. doi: 10.2302/kjm.11.105 - DOI
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
