

Total trans-obturator tape (TOT) removal; a case series including pain and urinary continence outcomes
- PMID: 35881175
- PMCID: PMC9314537
- DOI: 10.1007/s00192-022-05299-y
Total trans-obturator tape (TOT) removal; a case series including pain and urinary continence outcomes
Abstract
Introduction and hypothesis: For many years, mid-urethral mesh tape (MUT) was the gold-standard procedure for management of stress urinary incontinence (SUI). However, significant concerns were raised over its safety. We present a case series of total trans-obturator tape (TOT) removals, performed in a tertiary unit over a 3-year period. We aim to evaluate improvement of pain and change in urinary continence symptoms following mesh explantation.
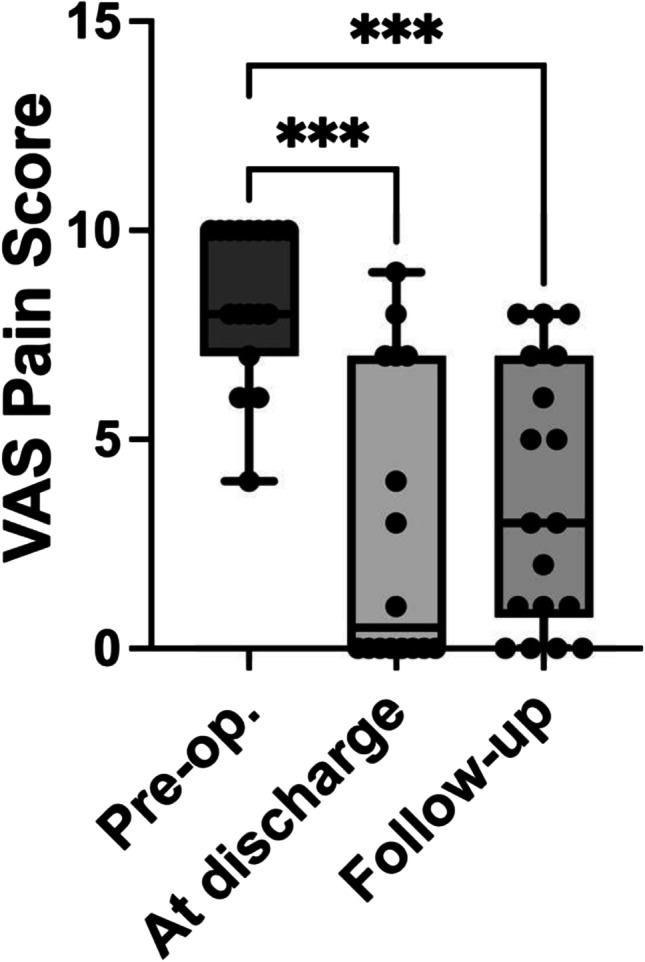
Methods: This is a retrospective case series of the outcomes of total TOT removal. Primary outcome is the change in pain scores following total removal, assessed preoperatively, at discharge and follow-up. Secondary outcomes were perioperative complications, including return to theatre, re-admission rates and incidence of worsening SUI and overactive bladder symptoms (OAB) postoperatively. Statistical analyses were performed using SPSS 27.0 package (IBM, Chicago, IL) and the GraphPad Prism 9 statistical packages.
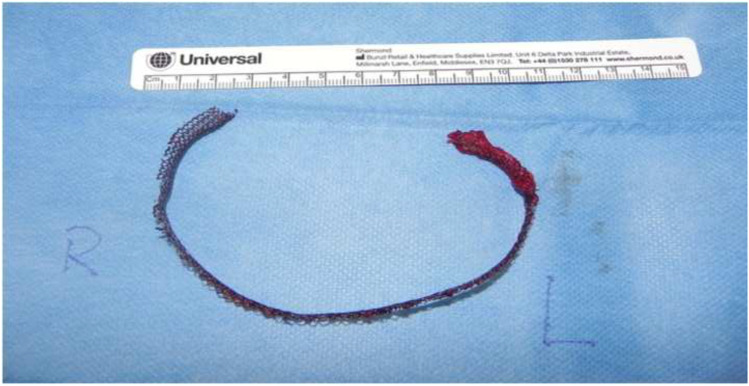
Results: Nineteen women were identified. Mean age was 52 years and mean BMI was 31. Indications for mesh removal were: chronic pain (95%), vaginal exposure (37%) and pelvic sepsis (5%). No patients had return to theatre. Median intraoperative blood loss was 200 ml (interquartile range [IQR]: 150-288). Mean length of mesh excised was 22 cm. Mean postoperative hospital stay was 2 days. At follow-up, most patients (72%) reported "improvement" of their mesh-related pain at follow-up, while 6% reported "worsening" of pain. Eighty-three per cent of patients reported worsening SUI, and 50% reported worsening OAB symptoms.
Conclusions: In the absence of sepsis, significant intraoperative complications are rare during total TOT removals. While 72% of patients reported improvement of their mesh-related pain, 6% still reported worsening pain after total mesh excision.
Keywords: Mesh complications; Mesh excision; Mesh removal; Pain; Stress urinary incontinence.
© 2022. The International Urogynecological Association.
Conflict of interest statement
Sami Shawer (SS), Vijna Boodhoo (VB), Oliver Licari (OL) and Stewart Pringle (SP): no conflict of interest for any of the authors.
Veenu Tyagi (VT): Executive member and/or member of the British Society of Urogynaecology (BSUG), the UK Continence Society (UKCS) and the Scottish Pelvic Floor Network (SPFN).
Vladimir Revicky (VR): Member of the British Society of Urogynaecology (BSUG) and the UK Continence Society (UKCS)
Karen Guerrero (KG): Executive member of the British Society of Urogynaecology (BSUG) and the UK Continence Society (UKCS). Chair of the RCOG sub-speciality training committee.
Figures
References
-
- Tennstedt SL, Fitzgerald MP, Nager CW, Xu Y, Zimmern P, Kraus S, Goode PS, Kusek JW, Borello-France D, Mallett V, Urinary Incontinence Treatment N. Quality of life in women with stress urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(5):543–549. doi: 10.1007/s00192-006-0188-5. - DOI - PubMed
-
- Government S. Transvaginal mesh implants independent review: interim report. 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
