

Feasibility of "cold" triangle robotic pancreatoduodenectomy
- PMID: 35881243
- PMCID: PMC9652209
- DOI: 10.1007/s00464-022-09411-7
Feasibility of "cold" triangle robotic pancreatoduodenectomy
Abstract
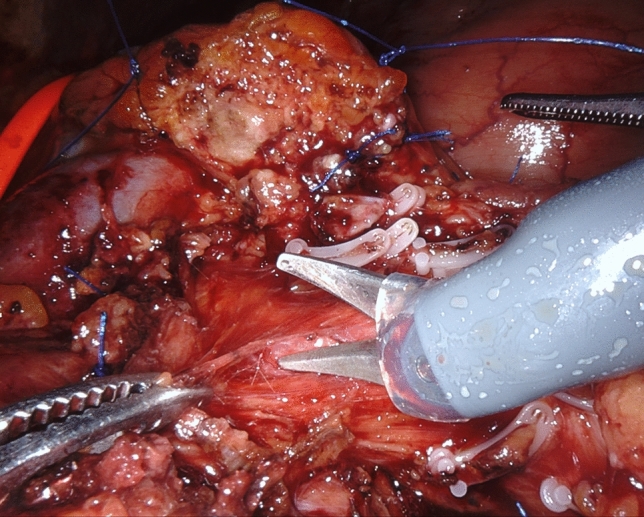
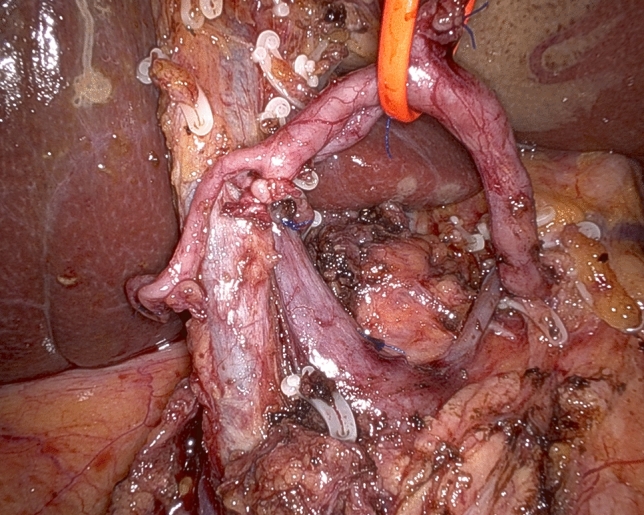
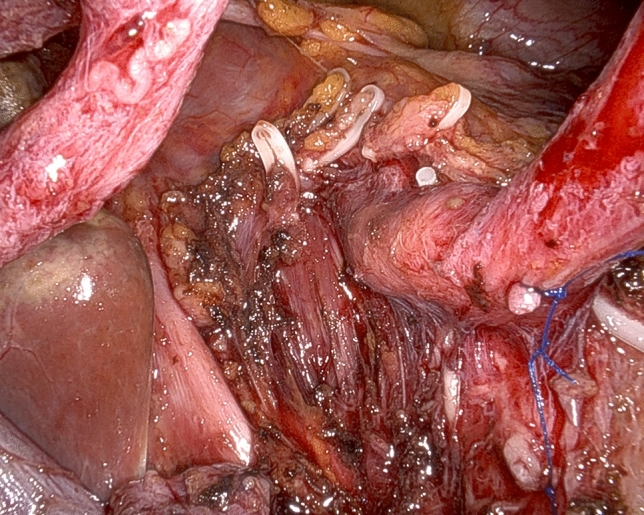
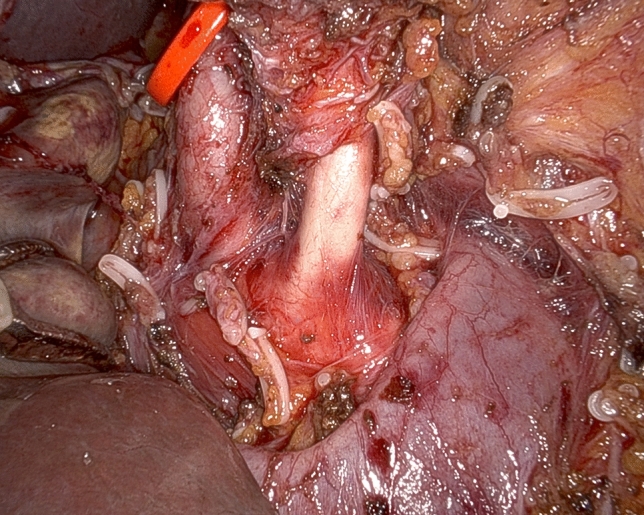
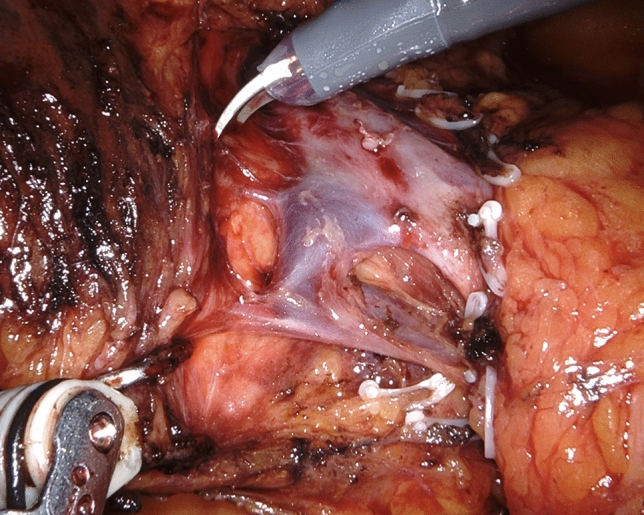
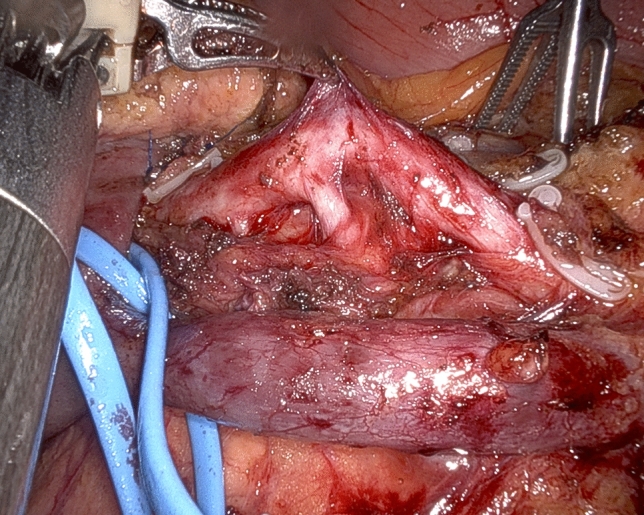
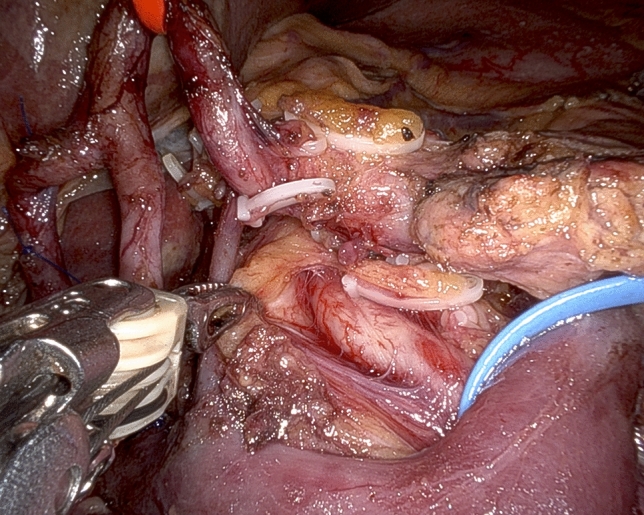
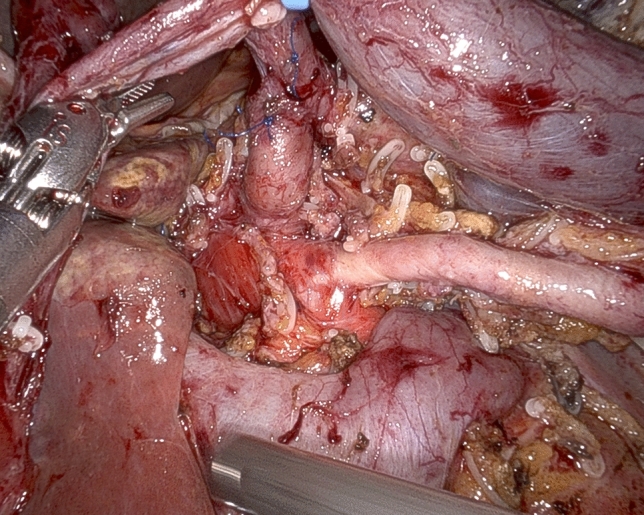
Background: Triangle pancreatoduodenectomy adds to the conventional procedure the en bloc removal of the retroperitoneal lympho-neural tissue included in the triangular area bounded by the common hepatic artery (CHA), the superior mesenteric artery (SMA), and the superior mesenteric vein/portal vein. We herein aim to show the feasibility of "cold" triangle robotic pancreaticoduodenectomy (C-Tr-RPD) for pancreatic cancer (PDAC).
Methods: Cold dissection corresponds to sharp arterial divestment performed using only the tips of robotic scissors. After division of the gastroduodenal artery, triangle dissection begins by lateral-to-medial divestment of the CHA and anterior-to-posterior clearance of the right side of the celiac trunk. Next, after a wide Kocher maneuver, the origin of the SMA, and the celiac trunk are identified. After mobilization of the first jejunal loop and attached mesentery, the SMA is identified at the level of the first jejunal vein and is divested along the right margin working in a distal-to-proximal direction. Vein resection and reconstruction can be performed as required. C-Tr-RPD was considered feasible if triangle dissection was successfully completed without conversion to open surgery or need to use energy devices. Postoperative complications and pathology results are presented in detail.
Results: One hundred twenty-seven consecutive C-Tr-RPDs were successfully performed. There were three conversions to open surgery (2.3%), because of pneumoperitoneum intolerance (n = 2) and difficult digestive reconstruction. Thirty-four patients (26.7%) required associated vascular procedures. No pseudoaneurysm of the gastroduodenal artery was observed. Twenty-eight patients (22.0%) developed severe postoperative complications (≥ grade III). Overall 90-day mortality was 7.1%, declining to 2.3% after completion of the learning curve. The median number of examined lymph nodes was 42 (33-51). The rate of R1 resection (7 margins < 1 mm) was 44.1%.
Conclusion: C-Tr-RPD is feasible, carries a risk of surgical complications commensurate to the magnitude of the procedure, and improves staging of PDAC.
Keywords: Mesopancreas; Pancreatic cancer; Pancreatoduodenectomy; Robot assisted; Robotic; Triangle.
© 2022. The Author(s).
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
