

Global economic burden of unmet surgical need for appendicitis
- PMID: 35881506
- PMCID: PMC10364778
- DOI: 10.1093/bjs/znac195
Global economic burden of unmet surgical need for appendicitis
Abstract
Background: There is a substantial gap in provision of adequate surgical care in many low- and middle-income countries. This study aimed to identify the economic burden of unmet surgical need for the common condition of appendicitis.
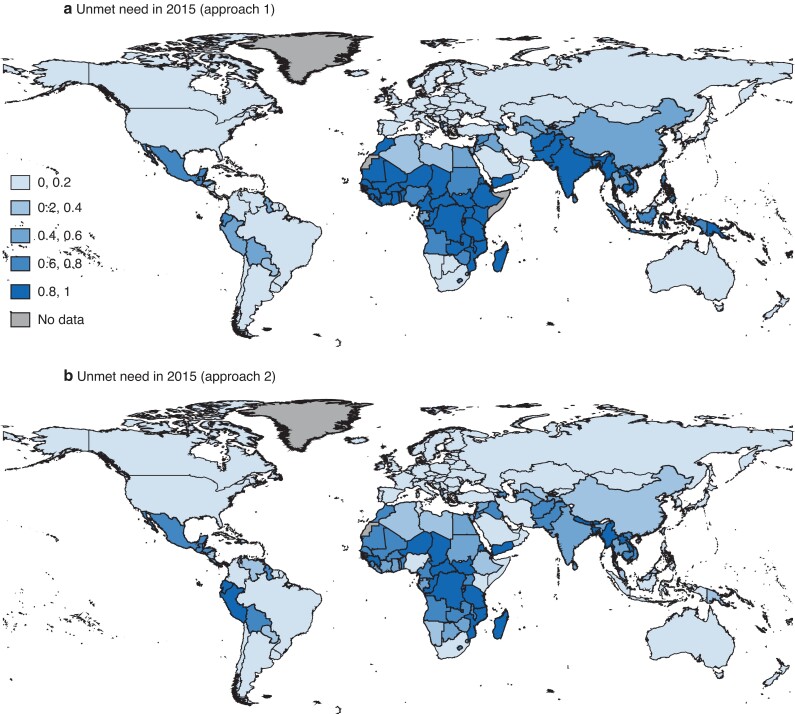
Methods: Data on the incidence of appendicitis from 170 countries and two different approaches were used to estimate numbers of patients who do not receive surgery: as a fixed proportion of the total unmet surgical need per country (approach 1); and based on country income status (approach 2). Indirect costs with current levels of access and local quality, and those if quality were at the standards of high-income countries, were estimated. A human capital approach was applied, focusing on the economic burden resulting from premature death and absenteeism.
Results: Excess mortality was 4185 per 100 000 cases of appendicitis using approach 1 and 3448 per 100 000 using approach 2. The economic burden of continuing current levels of access and local quality was US $92 492 million using approach 1 and $73 141 million using approach 2. The economic burden of not providing surgical care to the standards of high-income countries was $95 004 million using approach 1 and $75 666 million using approach 2. The largest share of these costs resulted from premature death (97.7 per cent) and lack of access (97.0 per cent) in contrast to lack of quality.
Conclusion: For a comparatively non-complex emergency condition such as appendicitis, increasing access to care should be prioritized. Although improving quality of care should not be neglected, increasing provision of care at current standards could reduce societal costs substantially.
© The Author(s) 2022. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures


References
-
- Meara JG, Leather AJM, Hagander L, Alkire BC, Alonso N, Ameh EA, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet 2015;386:569–624 - PubMed
-
- Biccard BM, Madiba TE, Kluyts HL, Munlemvo DM, Madzimbamuto FD, Basenero A et al. Perioperative patient outcomes in the African Surgical Outcomes Study: a 7-day prospective observational cohort study. Lancet 2018;391:1589–1598 - PubMed
-
- Bhangu A, Ademuyiwa AO, Aguilera ML, Alexander P, Al-Saqqa SW, Borda-Luque G et al. Surgical site infection after gastrointestinal surgery in high-income, middle-income, and low-income countries: a prospective, international, multicentre cohort study. Lancet Infect Diss 2018;18:516–525 - PMC - PubMed
-
- Hider P, Wilson L, Rose J, Weiser TG, Gruen R, Bickler SW. The role of facility-based surgical services in addressing the national burden of disease in New Zealand: an index of surgical incidence based on country-specific disease prevalence. Surgery 2015;158:44–54 - PubMed
-
- Chao TE, Sharma K, Mandigo M, Hagander L, Resch SC, Weiser TG et al. Cost-effectiveness of surgery and its policy implications for global health: a systematic review and analysis. Lancet Glob Health 2014;2:e334–e345 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
