

Presentation, Management, and Outcomes of Urinary Bladder Paraganglioma: Results From a Multicenter Study
- PMID: 35882219
- PMCID: PMC9516048
- DOI: 10.1210/clinem/dgac427
Presentation, Management, and Outcomes of Urinary Bladder Paraganglioma: Results From a Multicenter Study
Abstract
Context: Urinary bladder paraganglioma (UBPGL) is rare.
Objective: We aimed to characterize the presentation and outcomes of patients diagnosed with UBPGL.
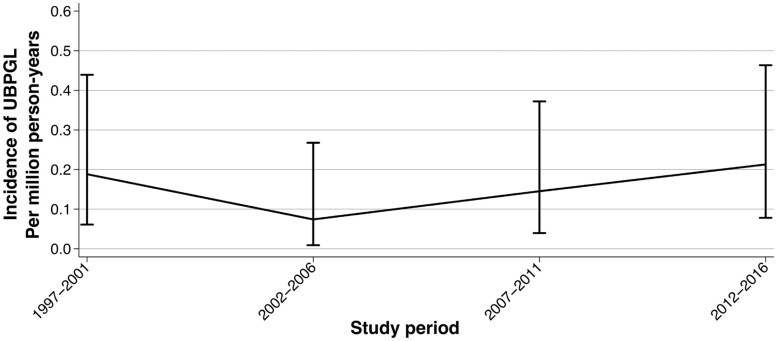
Methods: We conducted a multicenter study of consecutive patients with pathologically confirmed UBPGL evaluated between 1971 and 2021. Outcomes included repeat bladder surgery, metastases, and disease-specific mortality.
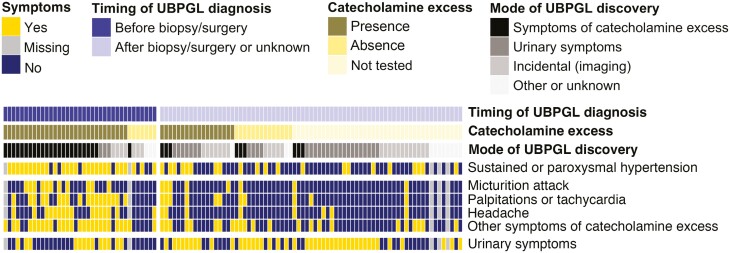
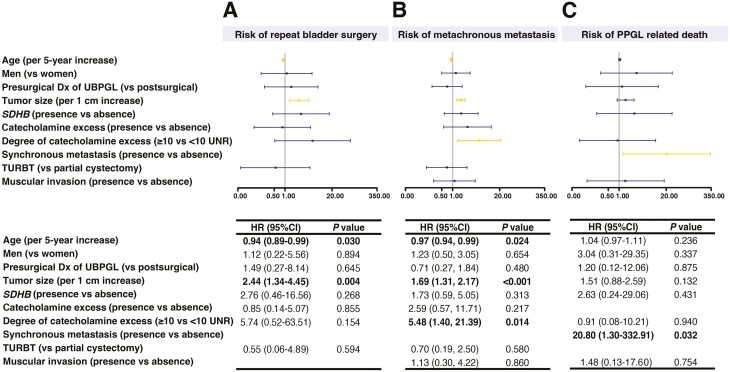
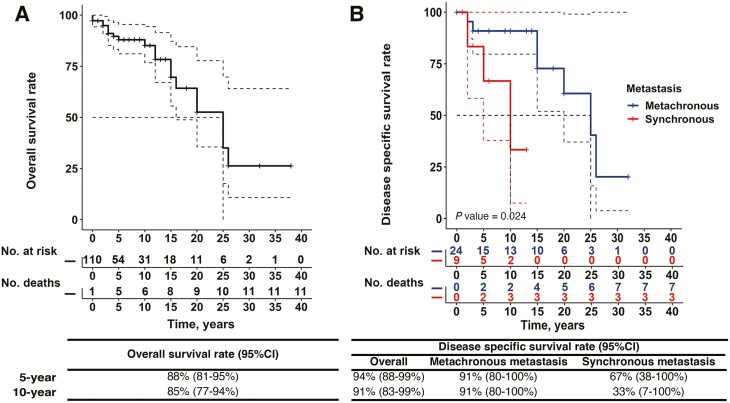
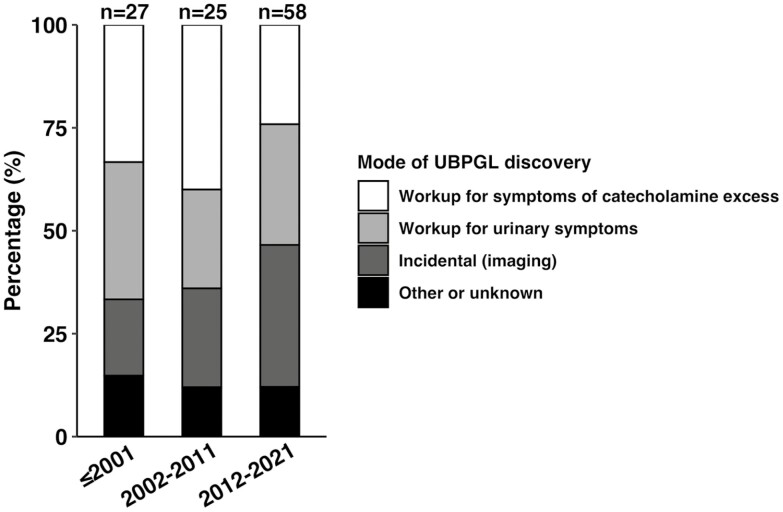
Results: Patients (n=110 total; n=56 [51%] women) were diagnosed with UBPGL at a median age of 50 years (interquartile range [IQR], 36-61 years). Median tumor size was 2 cm (IQR, 1-4 cm). UBPGL was diagnosed prior to biopsy in only 37 (34%), and only 69 (63%) patients had evaluation for catecholamine excess. In addition to the initial bladder surgery, 26 (25%) required multiple therapies, including repeat surgery in 10 (9%). Synchronous metastases were present in 9 (8%) patients, and 24 (22%) other patients with UBPGL developed metachronous metastases at a median of 4 years (IQR, 2-10 years) after the initial diagnosis. Development of metachronous metastases was associated with younger age (hazard ratio [HR] 0.97; 95% CI, 0.94-0.99), UBPGL size (HR 1.69; 95% CI, 1.31-2.17), and a higher degree of catecholamine excess (HR 5.48; 95% CI, 1.40-21.39). Disease-specific mortality was higher in patients with synchronous metastases (HR 20.80; 95% CI, 1.30-332.91). Choice of initial surgery, genetic association, sex, or presence of muscular involvement on pathology were not associated with development of metastases or mortality.
Conclusions: Only a minority of patients were diagnosed before biopsy/surgery, reflecting need for better diagnostic strategies. All patients with UBPGL should have lifelong monitoring for development of recurrence and metastases.
Keywords: catecholamine; diagnosis; micturition; prognosis.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Curras-Freixes M, Inglada-Perez L, Mancikova V, et al. . Recommendations for somatic and germline genetic testing of single pheochromocytoma and paraganglioma based on findings from a series of 329 patients. J Med Genet. 2015;52(10):647-656. - PubMed
-
- Erickson D, Kudva YC, Ebersold MJ, et al. . Benign paragangliomas: clinical presentation and treatment outcomes in 236 patients. J Clin Endocrinol Metab. 2001;86(11):5210-5216. - PubMed
-
- Schulte KM, Talat N, Galata G, et al. . Genetics and the clinical approach to paragangliomas. Horm Metab Res. 2014;46(13):964-973. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
