

Gestational diabetes mellitus and offspring's carotid intima-media thickness at birth: MySweetHeart Cohort study
- PMID: 35882452
- PMCID: PMC9330339
- DOI: 10.1136/bmjopen-2022-061649
Gestational diabetes mellitus and offspring's carotid intima-media thickness at birth: MySweetHeart Cohort study
Abstract
Objective: Hyperglycaemia during pregnancy is associated with cardiometabolic risks for the mother and the offspring. Mothers with gestational diabetes mellitus (GDM) have signs of subclinical atherosclerosis, including increased carotid intima-media thickness (CIMT). We assessed whether GDM is associated with increased CIMT in the offspring at birth.
Design and setting: MySweetHeart Cohort is a prospective cohort study conducted in Switzerland.
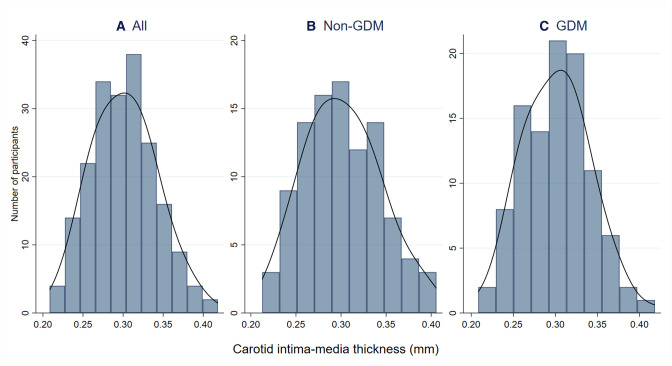
Participants, exposure and outcome measures: This work included pregnant women with and without GDM at 24-32 weeks of gestation and their singleton live-born offspring with data on the primary outcome of CIMT. GDM was diagnosed based on the criteria of the International Association of Diabetes and Pregnancy Study Groups. Offspring's CIMT was measured by ultrasonography after birth (range 1-19 days).
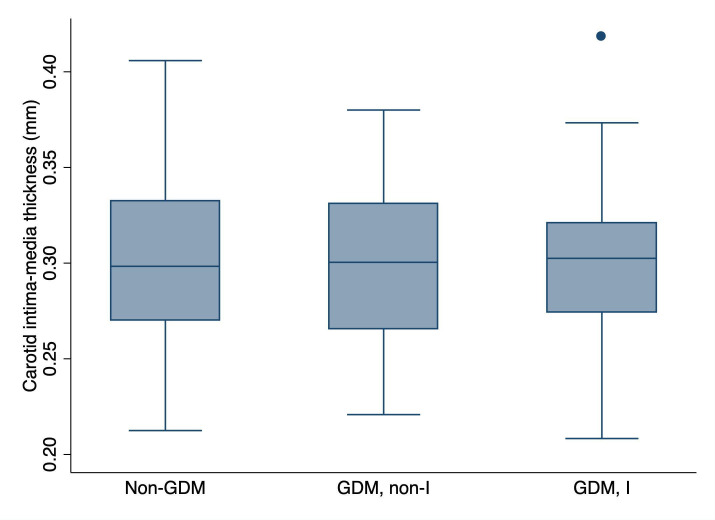
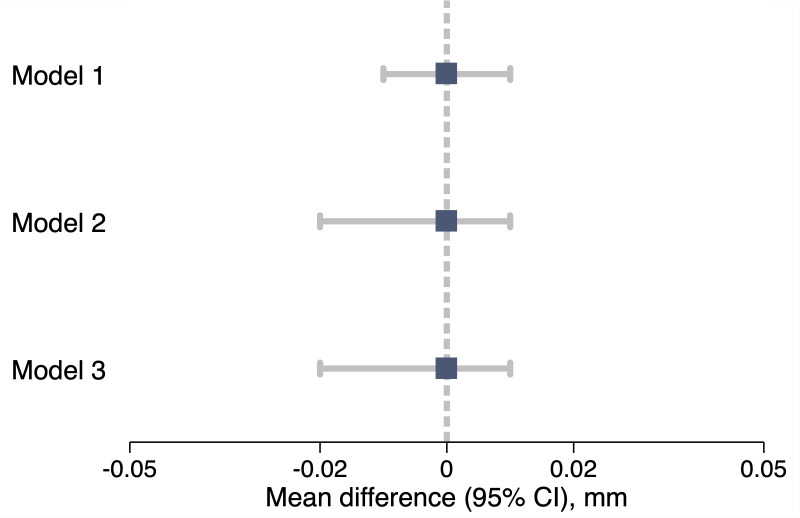
Results: Data on CIMT were available for 99 offspring of women without GDM and 101 offspring of women with GDM. Maternal age ranged from 18 to 47 years. Some 16% of women with GDM and 6% of women without GDM were obese. Smoking during pregnancy was more frequent among women with GDM (18%) than among those without GDM (4%). Neonatal characteristics were comparable between the two groups. The difference in CIMT between offspring of women with and without GDM was of 0.00 mm (95% CI -0.01 to 0.01; p=0.96) and remained similar on adjustment for potential confounding factors, such as maternal prepregnancy body mass index, maternal education, smoking during pregnancy, family history of diabetes, as well as offspring's sex, age, and body surface area (0.00 mm (95% CI -0.02 to 0.01; p=0.45)).
Conclusions: We found no evidence of increased CIMT in neonates exposed to GDM. A longer-term follow-up that includes additional vascular measures, such as endothelial function or arterial stiffness, may shed further light on the cardiovascular health trajectories in children born to mothers with GDM.
Trial registration number: NCT02872974; Pre-results.
Keywords: cardiac epidemiology; cardiovascular imaging; diabetes in pregnancy; neonatology; paediatric cardiology.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- International Diabetes Federation . IDF diabetes atlas. 9th edition. Brussels, Belgium: International Diabetes Federation, 2019.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical