

Machine Learning Models and Multiparametric Magnetic Resonance Imaging for the Prediction of Pathologic Response to Neoadjuvant Chemotherapy in Breast Cancer
- PMID: 35884572
- PMCID: PMC9317428
- DOI: 10.3390/cancers14143508
Machine Learning Models and Multiparametric Magnetic Resonance Imaging for the Prediction of Pathologic Response to Neoadjuvant Chemotherapy in Breast Cancer
Abstract
Background: Most breast cancer (BC) patients fail to achieve pathological complete response (pCR) after neoadjuvant chemotherapy (NAC). The aim of this study was to evaluate whether imaging features (perfusion/diffusion imaging biomarkers + radiomic features) extracted from pre-treatment multiparametric (mp)MRIs were able to predict, alone or in combination with clinical data, pCR to NAC.
Methods: Patients with stage II-III BC receiving NAC and undergoing breast mpMRI were retrospectively evaluated. Imaging features were extracted from mpMRIs performed before NAC. Three different machine learning models based on imaging features, clinical data or imaging features + clinical data were trained to predict pCR. Confusion matrices and performance metrics were obtained to assess model performance. Statistical analyses were conducted to evaluate differences between responders and non-responders.
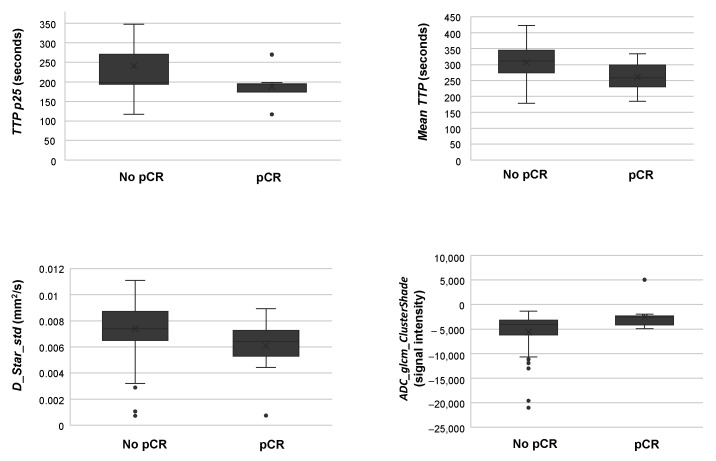
Results: Fifty-eight patients (median [range] age, 52 [45-58] years) were included, of whom 12 showed pCR. The combined model improved pCR prediction compared to clinical and imaging models, yielding 91.5% of accuracy with no false positive cases and only 17% false negative results. Changes in different parameters between responders and non-responders suggested a possible increase in vascularity and reduced tumour heterogeneity in patients with pCR, with the percentile 25th of time-to-peak (TTP), a classical perfusion parameter, being able to discriminate both groups in a 75% of the cases.
Conclusions: A combination of mpMRI-derived imaging features and clinical variables was able to successfully predict pCR to NAC. Specific patient profiles according to tumour vascularity and heterogeneity might explain pCR differences, where TTP could emerge as a putative surrogate marker for pCR.
Keywords: imaging biomarkers; machine learning; multiparametric MRI; radiomics.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Bear H.D., Anderson S., Brown A., Smith R., Mamounas E.P., Fisher B., Margolese R., Theoret H., Soran A., Wickerham D.L., et al. The effect on tumor response of adding sequential preoperative docetaxel to preoperative doxorubicin and cyclophosphamide: Preliminary results from National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J. Clin. Oncol. 2003;21:4165–4174. doi: 10.1200/JCO.2003.12.005. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
