

Differentiating False Positive Lesions from Clinically Significant Cancer and Normal Prostate Tissue Using VERDICT MRI and Other Diffusion Models
- PMID: 35885536
- PMCID: PMC9319485
- DOI: 10.3390/diagnostics12071631
Differentiating False Positive Lesions from Clinically Significant Cancer and Normal Prostate Tissue Using VERDICT MRI and Other Diffusion Models
Abstract
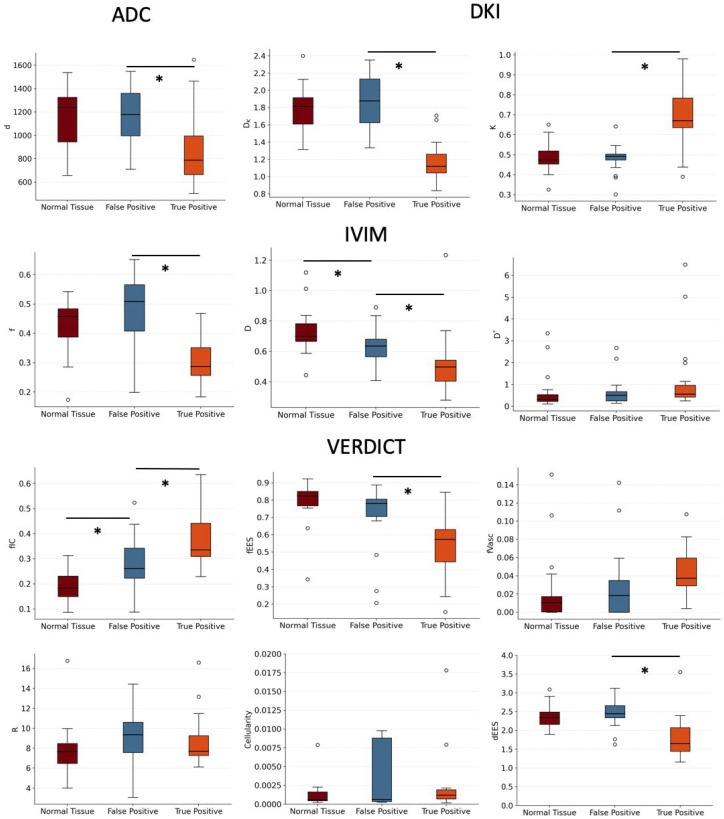
False positives on multiparametric MRIs (mp-MRIs) result in many unnecessary invasive biopsies in men with clinically insignificant diseases. This study investigated whether quantitative diffusion MRI could differentiate between false positives, true positives and normal tissue non-invasively. Thirty-eight patients underwent mp-MRI and Vascular, Extracellular and Restricted Diffusion for Cytometry in Tumors (VERDICT) MRI, followed by transperineal biopsy. The patients were categorized into two groups following biopsy: (1) significant cancer—true positive, 19 patients; (2) atrophy/inflammation/high-grade prostatic intraepithelial neoplasia (PIN)—false positive, 19 patients. The clinical apparent diffusion coefficient (ADC) values were obtained, and the intravoxel incoherent motion (IVIM), diffusion kurtosis imaging (DKI) and VERDICT models were fitted via deep learning. Significant differences (p < 0.05) between true positive and false positive lesions were found in ADC, IVIM perfusion fraction (f) and diffusivity (D), DKI diffusivity (DK) (p < 0.0001) and kurtosis (K) and VERDICT intracellular volume fraction (fIC), extracellular−extravascular volume fraction (fEES) and diffusivity (dEES) values. Significant differences between false positives and normal tissue were found for the VERDICT fIC (p = 0.004) and IVIM D. These results demonstrate that model-based diffusion MRI could reduce unnecessary biopsies occurring due to false positive prostate lesions and shows promising sensitivity to benign diseases.
Keywords: biophysical modeling; deep learning; diffusion MRI; false positives; prostate cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




Similar articles
-
Microstructural characterization of normal and malignant human prostate tissue with vascular, extracellular, and restricted diffusion for cytometry in tumours magnetic resonance imaging.Invest Radiol. 2015 Apr;50(4):218-27. doi: 10.1097/RLI.0000000000000115. Invest Radiol. 2015. PMID: 25426656
-
Intravoxel incoherent motion and diffusion kurtosis imaging and their machine-learning-based texture analysis for detection and assessment of prostate cancer severity at 3 T.NMR Biomed. 2024 Sep;37(9):e5144. doi: 10.1002/nbm.5144. Epub 2024 Mar 31. NMR Biomed. 2024. PMID: 38556777
-
VERDICT MRI for Prostate Cancer: Intracellular Volume Fraction versus Apparent Diffusion Coefficient.Radiology. 2019 May;291(2):391-397. doi: 10.1148/radiol.2019181749. Epub 2019 Apr 2. Radiology. 2019. PMID: 30938627 Free PMC article.
-
Multiparametric MRI in the Diagnosis of Prostate Cancer: Physical Foundations, Limitations, and Prospective Advances of Diffusion-Weighted MRI.Rofo. 2021 Apr;193(4):399-409. doi: 10.1055/a-1276-1773. Epub 2020 Dec 10. Rofo. 2021. PMID: 33302312 Review. English.
-
Intravoxel Incoherent Motion Diffusion-Weighted Imaging Used to Detect Prostate Cancer and Stratify Tumor Grade: A Meta-Analysis.Front Oncol. 2020 Sep 11;10:1623. doi: 10.3389/fonc.2020.01623. eCollection 2020. Front Oncol. 2020. PMID: 33042805 Free PMC article.
Cited by
-
Characteristic Mean Kurtosis Values in Simple Diffusion Kurtosis Imaging of Dentigerous Cysts.Diagnostics (Basel). 2023 Dec 7;13(24):3619. doi: 10.3390/diagnostics13243619. Diagnostics (Basel). 2023. PMID: 38132203 Free PMC article.
-
Giving the prostate the boost it needs: Spiral diffusion MRI using a high-performance whole-body gradient system for high b-values at short echo times.Magn Reson Med. 2025 Mar;93(3):1256-1272. doi: 10.1002/mrm.30351. Epub 2024 Nov 4. Magn Reson Med. 2025. PMID: 39497447 Free PMC article.
-
MRI-based virtual pathology of the prostate.MAGMA. 2024 Aug;37(4):709-720. doi: 10.1007/s10334-024-01163-w. Epub 2024 Jun 10. MAGMA. 2024. PMID: 38856839 Free PMC article. Review.
-
Precise Prostate Cancer Assessment Using IVIM-Based Parametric Estimation of Blood Diffusion from DW-MRI.Bioengineering (Basel). 2024 Jun 19;11(6):629. doi: 10.3390/bioengineering11060629. Bioengineering (Basel). 2024. PMID: 38927865 Free PMC article.
References
-
- Ahmed H.U., Bosaily A.E., Brown L.C., Gabe R., Kaplan R., Parmar M.K., Collaco-Moraes Y., Ward K., Hindley R.G., Freeman A., et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet. 2017;389:815–822. doi: 10.1016/S0140-6736(16)32401-1. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
