

Extra-Gynecological Pelvic Pathology: A Challenge in the Differential Diagnosis of the Female Pelvis
- PMID: 35885597
- PMCID: PMC9317774
- DOI: 10.3390/diagnostics12071693
Extra-Gynecological Pelvic Pathology: A Challenge in the Differential Diagnosis of the Female Pelvis
Abstract
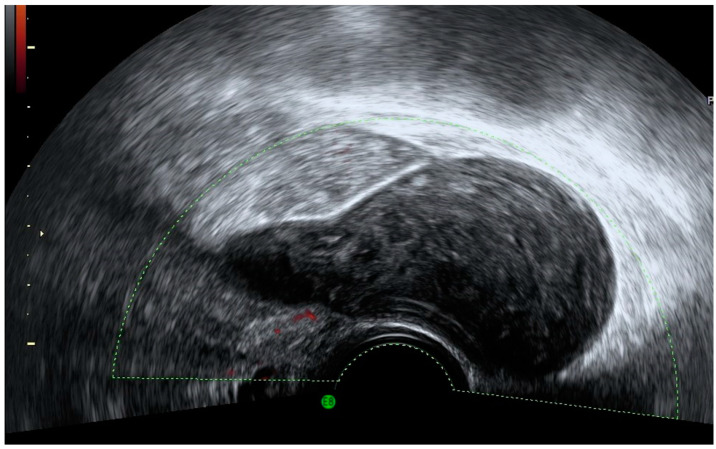
Ultrasound technology with or without color Doppler allows a real-time evaluation of the entire female pelvis including gynecologic and non-gynecological organs, as well as their pathology. As ultrasound is an accurate tool for gynecological diagnosis and is less invasive and less expensive than other techniques, it should be the first imaging modality used in the evaluation of the female pelvis. We present a miscellany of non-gynecological pelvic images observed during the realization of gynecological ultrasound. Transvaginal and transabdominal ultrasound is the first choice among diagnostic techniques for the study of the female pelvis, providing information about gynecological and extra-gynecological organs, allowing for an orientation toward the pathology of a specific organ or system as well as for additional tests to be performed that are necessary for definitive diagnosis.
Keywords: color Doppler; extra-gynecological disease; female pelvis; ultrasound.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




























References
-
- Beyer D., Schulte B., Kaiser C. Ultrasound diagnosis of the acute abdomen. Bildgebung. 1993;60:241–247. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
