

Exploring the Links between Obesity and Psoriasis: A Comprehensive Review
- PMID: 35886846
- PMCID: PMC9321445
- DOI: 10.3390/ijms23147499
Exploring the Links between Obesity and Psoriasis: A Comprehensive Review
Abstract
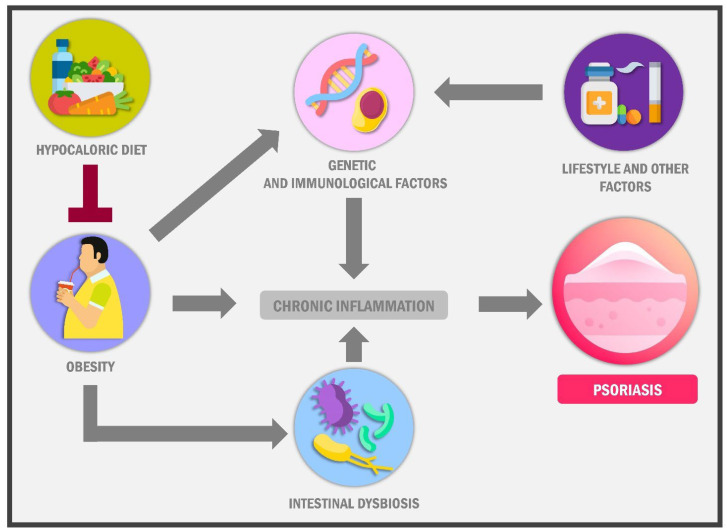
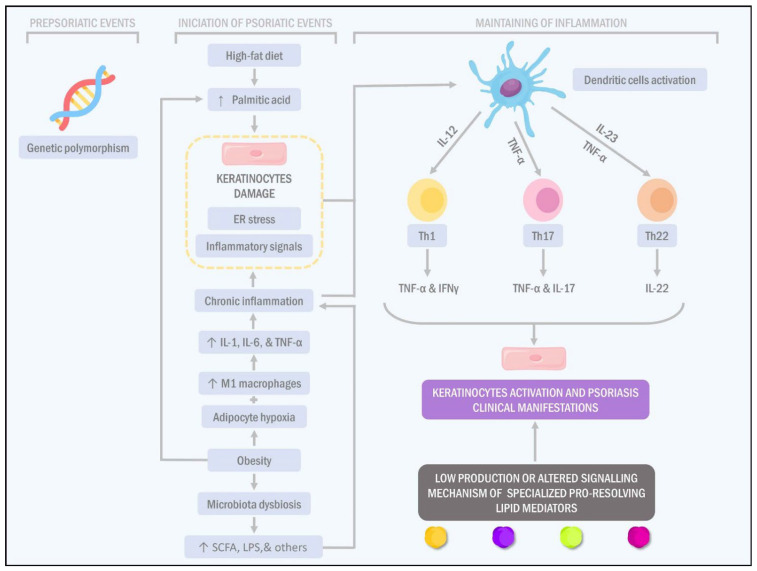
Obesity is a major public health issue worldwide since it is associated with the development of chronic comorbidities such as type 2 diabetes, dyslipidemias, atherosclerosis, some cancer forms and skin diseases, including psoriasis. Scientific evidence has indicated that the possible link between obesity and psoriasis may be multifactorial, highlighting dietary habits, lifestyle, certain genetic factors and the microbiome as leading factors in the progress of both pathologies because they are associated with a chronic pro-inflammatory state. Thus, inflammation management in obesity is a plausible target for psoriasis, not only because of the sick adipose tissue secretome profile but also due to the relationship of obesity with the rest of the immune derangements associated with psoriasis initiation and maintenance. Hence, this review will provide a general and molecular overview of the relationship between both pathologies and present recent therapeutic advances in treating this problem.
Keywords: adipokines; body mass index; cytokines; inflammation; microbiota; obesity; psoriasis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
