

Predictive Value of HAS-BLED Score Regarding Bleeding Events and Graft Survival following Renal Transplantation
- PMID: 35887788
- PMCID: PMC9319563
- DOI: 10.3390/jcm11144025
Predictive Value of HAS-BLED Score Regarding Bleeding Events and Graft Survival following Renal Transplantation
Abstract
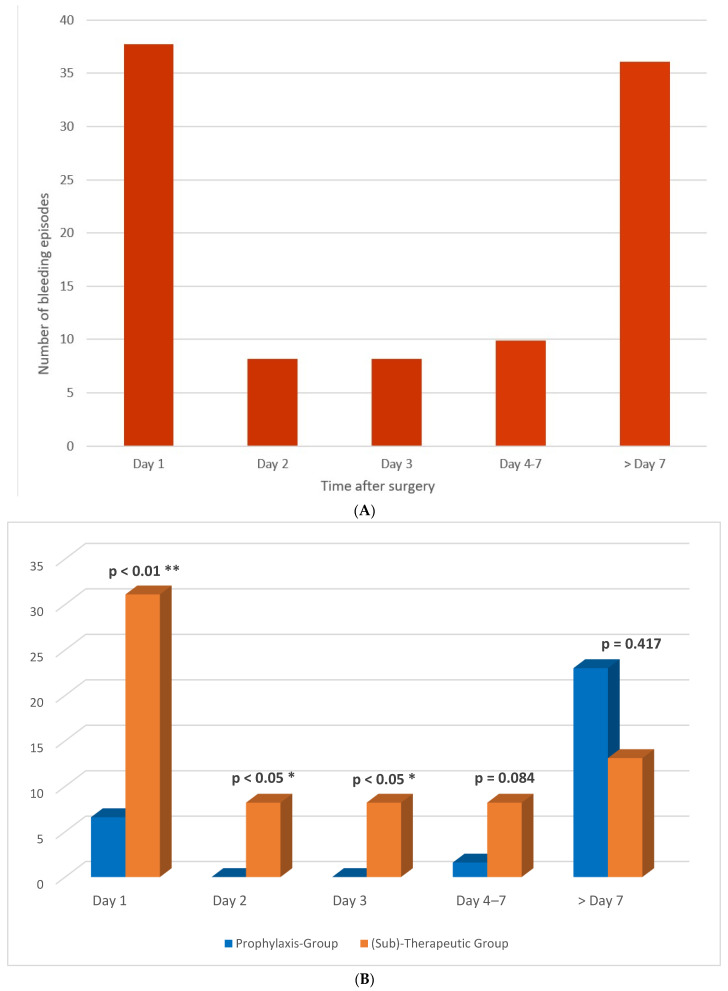
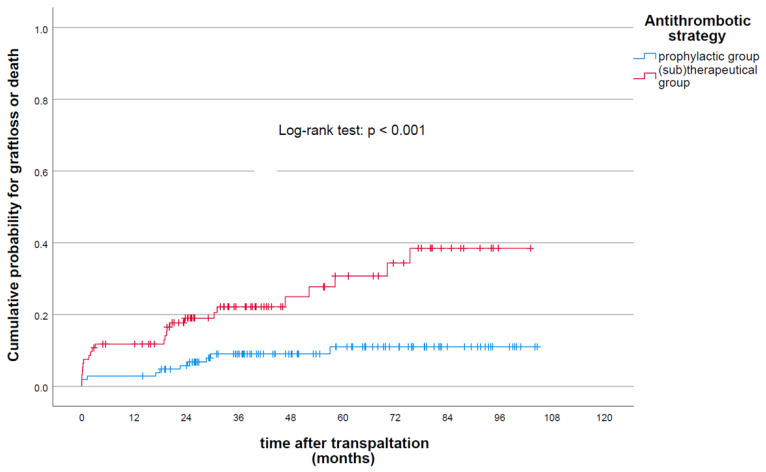
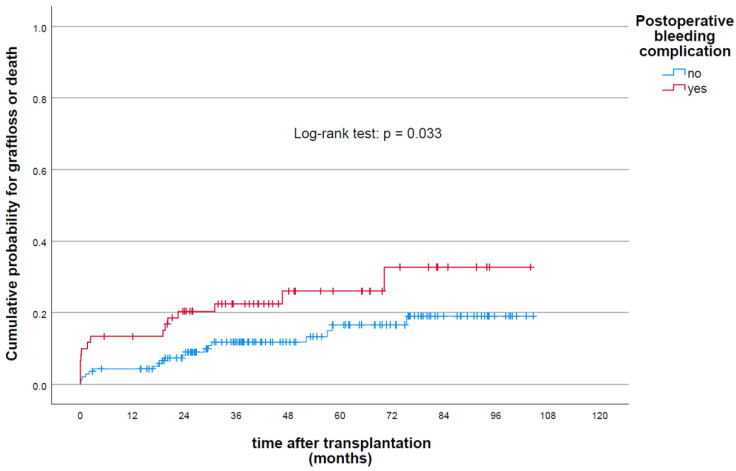
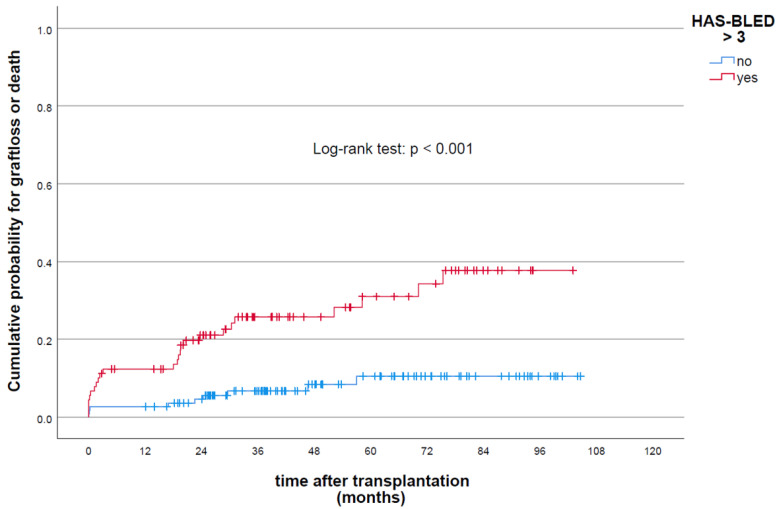
Objective: Due to the high prevalence and incidence of cardio- and cerebrovascular diseases among dialysis-dependent patients with end-stage renal disease (ERSD) scheduled for kidney transplantation (KT), the use of antiplatelet therapy (APT) and/or anticoagulant drugs in this patient population is common. However, these patients share a high risk of complications, either due to thromboembolic or bleeding events, which makes adequate peri- and post-transplant anticoagulation management challenging. Predictive clinical models, such as the HAS-BLED score developed for predicting major bleeding events in patients under anticoagulation therapy, could be helpful tools for the optimization of antithrombotic management and could reduce peri- and postoperative morbidity and mortality. Methods: Data from 204 patients undergoing kidney transplantation (KT) between 2011 and 2018 at the University Hospital Leipzig were retrospectively analyzed. Patients were stratified and categorized postoperatively into the prophylaxis group (group A)—patients without pretransplant anticoagulation/antiplatelet therapy and receiving postoperative heparin in prophylactic doses—and into the (sub)therapeutic group (group B)—patients with postoperative continued use of pretransplant antithrombotic medication used (sub)therapeutically. The primary outcome was the incidence of postoperative bleeding events, which was evaluated for a possible association with the use of antithrombotic therapy. Secondary analyses were conducted for the associations of other potential risk factors, specifically the HAS-BLED score, with allograft outcome. Univariate and multivariate logistic regression as well as a Cox proportional hazard model were used to identify risk factors for long-term allograft function, outcome and survival. The calibration and prognostic accuracy of the risk models were evaluated using the Hosmer−Lemshow test (HLT) and the area under the receiver operating characteristic curve (AUC) model. Results: In total, 94 of 204 (47%) patients received (sub)therapeutic antithrombotic therapy after transplantation and 108 (53%) patients received prophylactic antithrombotic therapy. A total of 61 (29%) patients showed signs of postoperative bleeding. The incidence (p < 0.01) and timepoint of bleeding (p < 0.01) varied significantly between the different antithrombotic treatment groups. After applying multivariate analyses, pre-existing cardiovascular disease (CVD) (OR 2.89 (95% CI: 1.02−8.21); p = 0.04), procedure-specific complications (blood loss (OR 1.03 (95% CI: 1.0−1.05); p = 0.014), Clavien−Dindo classification > grade II (OR 1.03 (95% CI: 1.0−1.05); p = 0.018)), HAS-BLED score (OR 1.49 (95% CI: 1.08−2.07); p = 0.018), vit K antagonists (VKA) (OR 5.89 (95% CI: 1.10−31.28); p = 0.037), the combination of APT and therapeutic heparin (OR 5.44 (95% CI: 1.33−22.31); p = 0.018) as well as postoperative therapeutic heparin (OR 3.37 (95% CI: 1.37−8.26); p < 0.01) were independently associated with an increased risk for bleeding. The intraoperative use of heparin, prior antiplatelet therapy and APT in combination with prophylactic heparin was not associated with increased bleeding risk. Higher recipient body mass index (BMI) (OR 0.32 per 10 kg/m2 increase in BMI (95% CI: 0.12−0.91); p = 0.023) as well as living donor KT (OR 0.43 (95% CI: 0.18−0.94); p = 0.036) were associated with a decreased risk for bleeding. Regarding bleeding events and graft failure, the HAS-BLED risk model demonstrated good calibration (bleeding and graft failure: HLT: chi-square: 4.572, p = 0.802, versus chi-square: 6.52, p = 0.18, respectively) and moderate predictive performance (bleeding AUC: 0.72 (0.63−0.79); graft failure: AUC: 0.7 (0.6−0.78)). Conclusions: In our current study, we could demonstrate the HAS-BLED risk score as a helpful tool with acceptable predictive accuracy regarding bleeding events and graft failure following KT. The intensified monitoring and precise stratification/assessment of bleeding risk factors may be helpful in identifying patients at higher risks of bleeding, improved individualized anticoagulation decisions and choices of antithrombotic therapy in order to optimize outcome after kidney transplantation.
Keywords: HAS-BLED score; anticoagulation; antiplatelet therapy; cardiovascular disease; kidney transplantation.
Conflict of interest statement
The authors declare that they have no competing interests or conflict of interest.
Figures
Similar articles
-
The Role of Innate Immune Cells in the Prediction of Early Renal Allograft Injury Following Kidney Transplantation.J Clin Med. 2022 Oct 18;11(20):6148. doi: 10.3390/jcm11206148. J Clin Med. 2022. PMID: 36294469 Free PMC article.
-
Relation of the HAS-BLED bleeding risk score to major bleeding, cardiovascular events, and mortality in anticoagulated patients with atrial fibrillation.Circ Arrhythm Electrophysiol. 2012 Apr;5(2):312-8. doi: 10.1161/CIRCEP.111.967000. Epub 2012 Feb 7. Circ Arrhythm Electrophysiol. 2012. PMID: 22319005
-
Interventions for preventing thrombosis in solid organ transplant recipients.Cochrane Database Syst Rev. 2021 Mar 15;3(3):CD011557. doi: 10.1002/14651858.CD011557.pub2. Cochrane Database Syst Rev. 2021. PMID: 33720396 Free PMC article.
-
Correlation of Different Serum Biomarkers with Prediction of Early Pancreatic Graft Dysfunction Following Simultaneous Pancreas and Kidney Transplantation.J Clin Med. 2022 May 3;11(9):2563. doi: 10.3390/jcm11092563. J Clin Med. 2022. PMID: 35566689 Free PMC article.
-
Assessment of bleeding risk of interventional techniques: a best evidence synthesis of practice patterns and perioperative management of anticoagulant and antithrombotic therapy.Pain Physician. 2013 Apr;16(2 Suppl):SE261-318. Pain Physician. 2013. PMID: 23615893 Review.
References
-
- Berg T.A.J., Minnee R.C., Lisman T., Nieuwenhuijs-Moeke G.J., Wetering J., Bakker S.J.L., Pol R.A. Perioperative antithrombotic therapy does not increase the incidence of early postoperative thromboembolic complications and bleeding in kidney transplantation—A retrospective study. Transpl. Int. 2019;32:418–430. doi: 10.1111/tri.13387. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
