

Thoracic Endovascular Aortic Repair (TEVAR) First in Patients with Lower Limb Ischemia in Complicated Type B Aortic Dissection: Clinical Outcome and Morphology
- PMID: 35887918
- PMCID: PMC9320233
- DOI: 10.3390/jcm11144154
Thoracic Endovascular Aortic Repair (TEVAR) First in Patients with Lower Limb Ischemia in Complicated Type B Aortic Dissection: Clinical Outcome and Morphology
Abstract
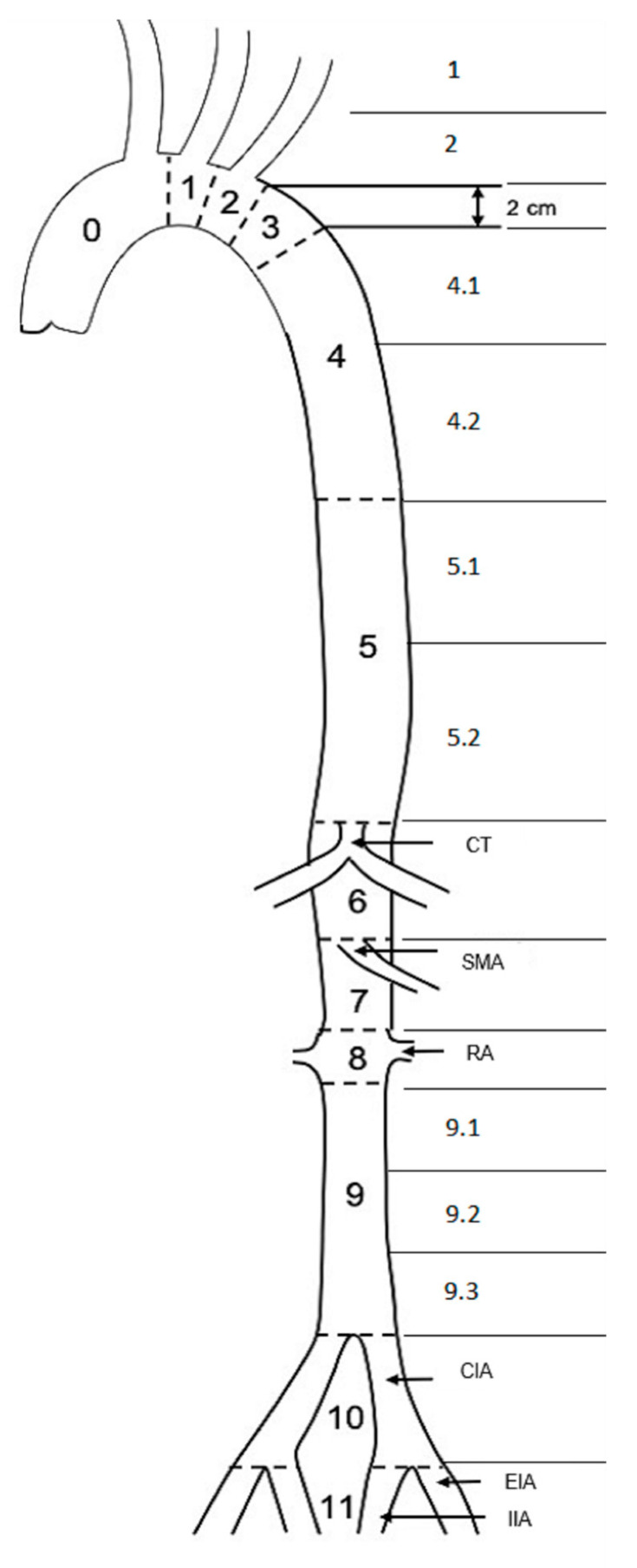
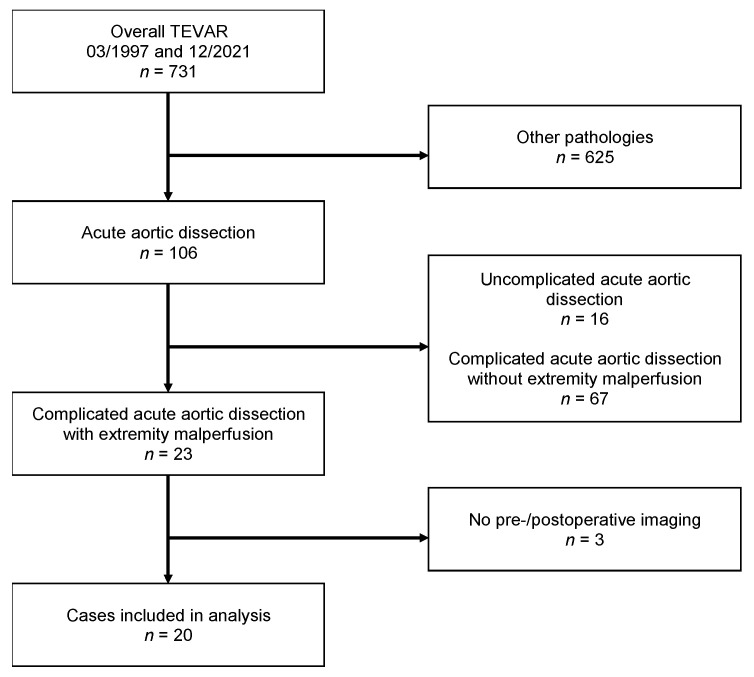
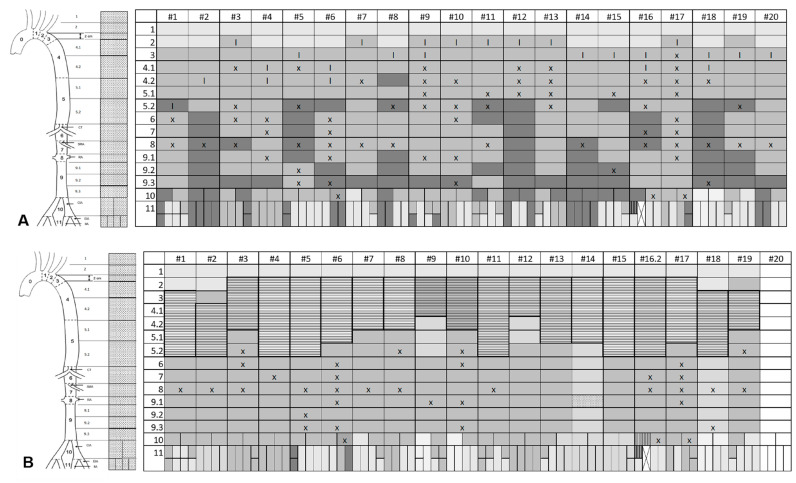
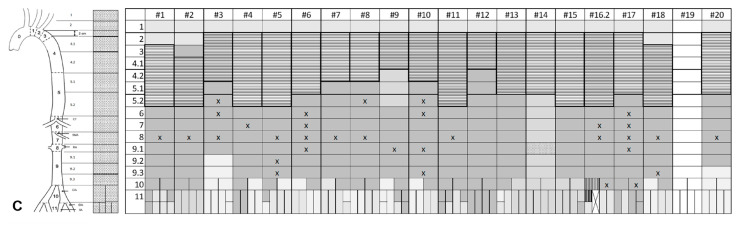
Acute Type B aortic dissection (TBAD) can cause organ malperfusion, e.g., lower limb ischemia (LLI). Thoracic endovascular aortic repair (TEVAR) represents the standard treatment for complicated TBAD; however, with respect to LLI, data is scant. The aim of this study was to investigate clinical and morphological outcomes in patients with complicated TBAD and LLI managed with a "TEVAR-first" policy. Between March 1997 and December 2021, 731 TEVAR-procedures were performed, including 106 TBAD-cases. Cases with TBAD + LLI were included in this retrospective analysis. Study endpoints were morphological/clinical success of TEVAR, regarding aortic and extremity-related outcome, including extremity-related adjunct procedures (erAP) during a median FU of 28.68 months. A total of 20/106 TBAD-cases (18.8%, 32-82 years, 7 women) presented with acute LLI (12/20 Rutherford class IIb/III). In 15/20 cases, true lumen-collapse (TLC) was present below the aortic bifurcation. In 16/20 cases, TEVAR alone resolved LLI. In the remaining four cases, erAP was necessary. A morphological analysis showed a relation between lower starting point and lesser extent of TLC and TEVAR success. No extremity-related reinterventions and only one major amputation was needed. The data strongly suggest that aTEVAR-first-strategy for treating TBAD with LLI is reasonable. Morphological parameters might be of importance to anticipate the failure of TEVAR alone.
Keywords: TEVAR; aortic dissection; complicated type B dissection; extremity malperfusion; lower limb ischemia; malperfusion; thoracic endovascular repair.
Conflict of interest statement
D.B. is a consultant for W.L. Gore & Associates, Arsenal Medical, Brainlab AG, Cook Medical, Endologix LLC, Medtronic GmbH, and a member of the advisory board of Brainlab AG, Cook Medical, Endologix LLC, Medtronic GmbH, W.L. Gore & Associates, and Siemens AG and has received speaker honoraria and educational and research grants from W.L. Gore & Associates, Cook Medical, Endologix LLC, Medtronic GmbH, Siemens Ag, and Getinge GmbH. M.S.B. has received speaker honoraria from W.L. Gore & Associates. A.S.P. has received speaker honoraria from Medtronic GmbH and Johnson & Johnson Medical GmbH and a travel grant from the 41st Charing Cross Symposium 2019, 15–18 April 2019. All other authors declare no conflict of interest.
Figures
Similar articles
-
Impact of aortic visceral branch vessel interventions on the postoperative outcomes of thoracic endovascular aortic repair for type B aortic dissection complicated with visceral malperfusion.J Vasc Surg. 2025 Sep;82(3):780-792.e2. doi: 10.1016/j.jvs.2025.05.003. Epub 2025 May 9. J Vasc Surg. 2025. PMID: 40348289
-
Management of acute type B aortic dissections and acute limb ischemia.J Cardiovasc Surg (Torino). 2011 Aug;52(4):507-17. J Cardiovasc Surg (Torino). 2011. PMID: 21792158 Review.
-
Masquerade presentation of acute type B aortic dissection as isolated acute limb ischaemia treated with endovascular fenestration with angioplasty: A case report.Int J Surg Case Rep. 2022 Mar;92:106857. doi: 10.1016/j.ijscr.2022.106857. Epub 2022 Feb 25. Int J Surg Case Rep. 2022. PMID: 35248883 Free PMC article.
-
Evaluation of Thoracic Endovascular Repair for the Treatment of Type B Aortic Dissection Complicated by Malperfusion.Ann Vasc Dis. 2024 Sep 25;17(3):248-254. doi: 10.3400/avd.oa.24-00036. Epub 2024 Jun 18. Ann Vasc Dis. 2024. PMID: 39359567 Free PMC article.
-
Lower limb malperfusion in type B aortic dissection: a systematic review.Ann Cardiothorac Surg. 2014 Jul;3(4):351-67. doi: 10.3978/j.issn.2225-319X.2014.07.05. Ann Cardiothorac Surg. 2014. PMID: 25133098 Free PMC article. Review.
Cited by
-
Calpain inhibition as a novel therapeutic strategy for aortic dissection with acute lower extremity ischemia.Mol Med. 2025 Apr 21;31(1):144. doi: 10.1186/s10020-025-01212-7. Mol Med. 2025. PMID: 40259242 Free PMC article.
References
-
- Riambau V., Böckler D., Brunkwall J., Cao P., Chiesa R., Coppi G., Czerny M., Fraedrich G., Haulon S., Jacobs M.J., et al. Editor’s Choice-Management of Descending Thoracic Aorta Diseases: Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS) Eur. J. Vasc. Endovasc. Surg. 2017;53:4–52. doi: 10.1016/j.ejvs.2016.06.005. - DOI - PubMed
-
- MacGillivray T.E., Gleason T.G., Patel H.J., Aldea G.S., Bavaria J.E., Beaver T.M., Chen E.P., Czerny M., Estrera A.L., Firestone S., et al. The Society of Thoracic Surgeons/American Association for Thoracic Surgery Clinical Practice Guidelines on the Management of Type B Aortic Dissection. Ann. Thorac. Surg. 2022;113:1073–1092. doi: 10.1016/j.athoracsur.2021.11.002. - DOI - PubMed
-
- Fattori R., Tsai T.T., Myrmel T., Evangelista A., Cooper J.V., Trimarchi S., Li J., Lovato L., Kische S., Eagle K.A., et al. Complicated acute type B dissection: Is surgery still the best option?: A report from the International Registry of Acute Aortic Dissection. JACC Cardiovasc. Interv. 2008;1:395–402. doi: 10.1016/j.jcin.2008.04.009. - DOI - PubMed
-
- Zeeshan A., Woo E.Y., Bavaria J.E., Fairman R.M., Desai N.D., Pochettino A., Szeto W.Y. Thoracic endovascular aortic repair for acute complicated type B aortic dissection: Superiority relative to conventional open surgical and medical therapy. J. Thorac. Cardiovasc. Surg. 2010;140((Suppl. S6)):S109–S115; discussion S42–S46. doi: 10.1016/j.jtcvs.2010.06.024. - DOI - PubMed
-
- Suzuki T., Mehta R.H., Ince H., Nagai R., Sakomura Y., Weber F., Sumiyoshi T., Bossone E., Trimarchi S., Cooper J.V., et al. Clinical profiles and outcomes of acute type B aortic dissection in the current era: Lessons from the International Registry of Aortic Dissection (IRAD) Circulation. 2003;108((Suppl. S1)):II312–II317. doi: 10.1161/01.cir.0000087386.07204.09. - DOI - PubMed
LinkOut - more resources
Full Text Sources
