

Development and Internal Validation of a New Prognostic Model Powered to Predict 28-Day All-Cause Mortality in ICU COVID-19 Patients-The COVID-SOFA Score
- PMID: 35887924
- PMCID: PMC9323813
- DOI: 10.3390/jcm11144160
Development and Internal Validation of a New Prognostic Model Powered to Predict 28-Day All-Cause Mortality in ICU COVID-19 Patients-The COVID-SOFA Score
Abstract
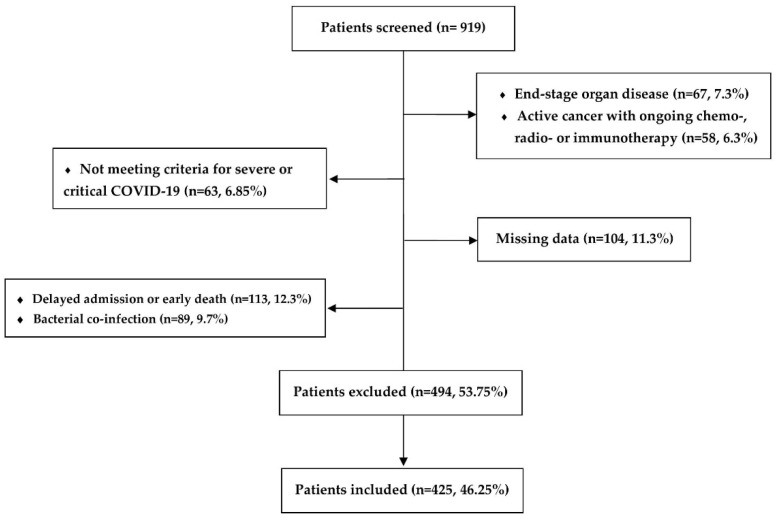
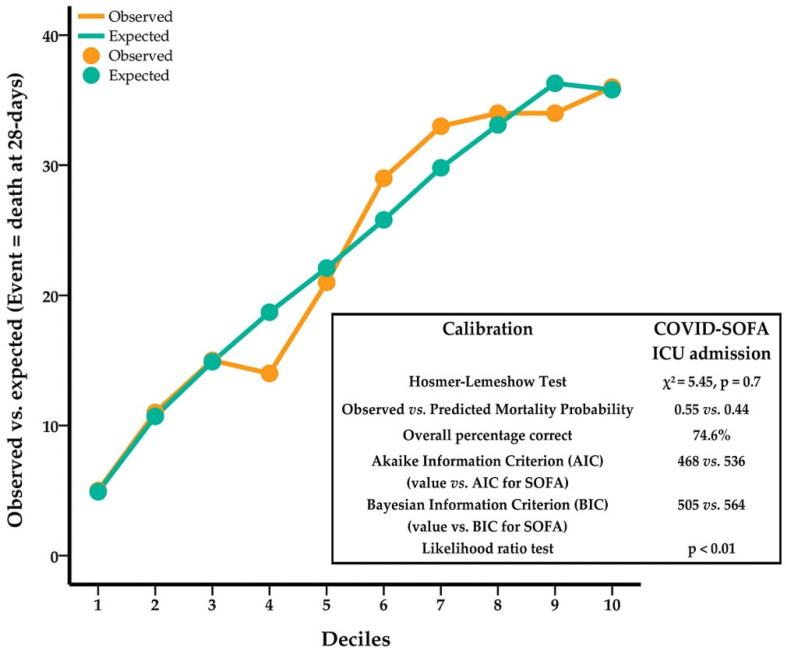
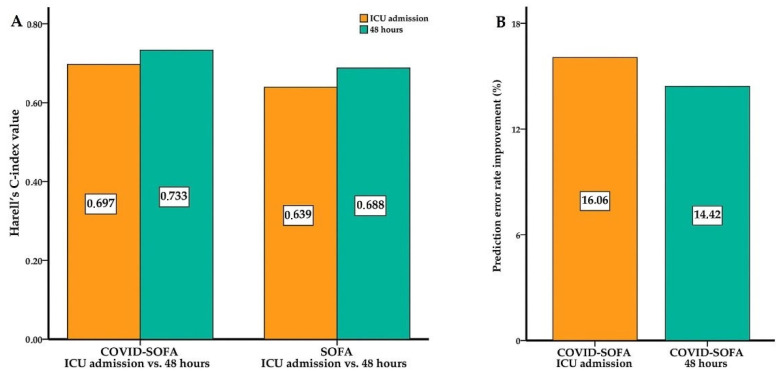
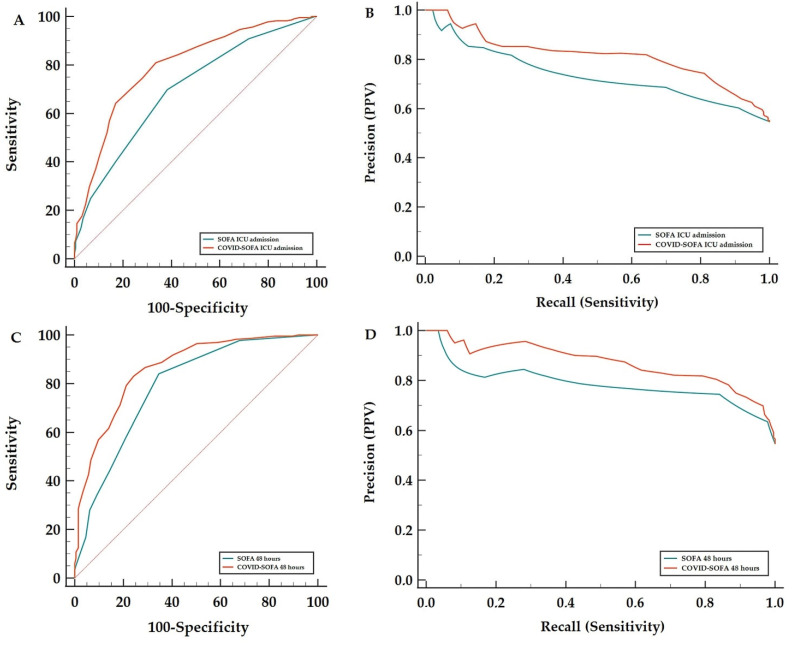
Background: The sequential organ failure assessment (SOFA) score has poor discriminative ability for death in severely or critically ill patients with Coronavirus disease 2019 (COVID-19) requiring intensive care unit (ICU) admission. Our aim was to create a new score powered to predict 28-day mortality. Methods: Retrospective, observational, bicentric cohort study including 425 patients with COVID-19 pneumonia, acute respiratory failure and SOFA score ≥ 2 requiring ICU admission for ≥72 h. Factors with independent predictive value for 28-day mortality were identified after stepwise Cox proportional hazards (PH) regression. Based on the regression coefficients, an equation was computed representing the COVID-SOFA score. Discriminative ability was tested using receiver operating characteristic (ROC) analysis, concordance statistics and precision-recall curves. This score was internally validated. Results: Median (Q1−Q3) age for the whole sample was 64 [55−72], with 290 (68.2%) of patients being male. The 28-day mortality was 54.58%. After stepwise Cox PH regression, age, neutrophil-to-lymphocyte ratio (NLR) and SOFA score remained in the final model. The following equation was computed: COVID-SOFA score = 10 × [0.037 × Age + 0.347 × ln(NLR) + 0.16 × SOFA]. Harrell’s C-index for the COVID-SOFA score was higher than the SOFA score alone for 28-day mortality (0.697 [95% CI; 0.662−0.731] versus 0.639 [95% CI: 0.605−0.672]). Subsequently, the prediction error rate was improved up to 16.06%. Area under the ROC (AUROC) was significantly higher for the COVID-SOFA score compared with the SOFA score for 28-day mortality: 0.796 [95% CI: 0.755−0.833] versus 0.699 [95% CI: 0.653−0.742, p < 0.001]. Better predictive value was observed with repeated measurement at 48 h after ICU admission. Conclusions: The COVID-SOFA score is better than the SOFA score alone for 28-day mortality prediction. Improvement in predictive value seen with measurements at 48 h after ICU admission suggests that the COVID-SOFA score can be used in a repetitive manner. External validation is required to support these results.
Keywords: ARDS; COVID-19; ICU; NLR; SARS-CoV-2; SOFA; mortality; neutrophil-to-lymphocyte ratio; prognostic score.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Singer M., Deutschman C.S., Seymour C.W., Shankar-Hari M., Annane D., Bauer M., Bellomo R., Bernard G.R., Chiche J.-D., Coopersmith C.M., et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) JAMA. 2016;315:801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
-
- Karakike E., Giamarellos-Bourboulis E.J., Kyprianou M., Fleischmann-Struzek C., Pletz M.W., Netea M.G., Reinhart K., Kyriazopoulou E. Coronavirus Disease 2019 as Cause of Viral Sepsis: A Systematic Review and Meta-Analysis. Crit. Care Med. 2021;49:2042. doi: 10.1097/CCM.0000000000005195. - DOI - PMC - PubMed
-
- Antommaria A.H.M., Gibb T.S., McGuire A.L., Wolpe P.R., Wynia M.K., Applewhite M.K., Caplan A., Diekema D.S., Hester D.M., Lehmann L.S., et al. Ventilator Triage Policies during the COVID-19 Pandemic at U.S. Hospitals Associated with Members of the Association of Bioethics Program Directors. Ann. Intern. Med. 2020;173:188–194. doi: 10.7326/M20-1738. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
