

Real-World Safety, Effectiveness, and Patient-Reported Outcomes in Patients with Chronic Hepatitis C Virus Infection Treated with Glecaprevir/Pibrentasvir: Updated Data from the German Hepatitis C-Registry (DHC-R)
- PMID: 35891520
- PMCID: PMC9318383
- DOI: 10.3390/v14071541
Real-World Safety, Effectiveness, and Patient-Reported Outcomes in Patients with Chronic Hepatitis C Virus Infection Treated with Glecaprevir/Pibrentasvir: Updated Data from the German Hepatitis C-Registry (DHC-R)
Abstract
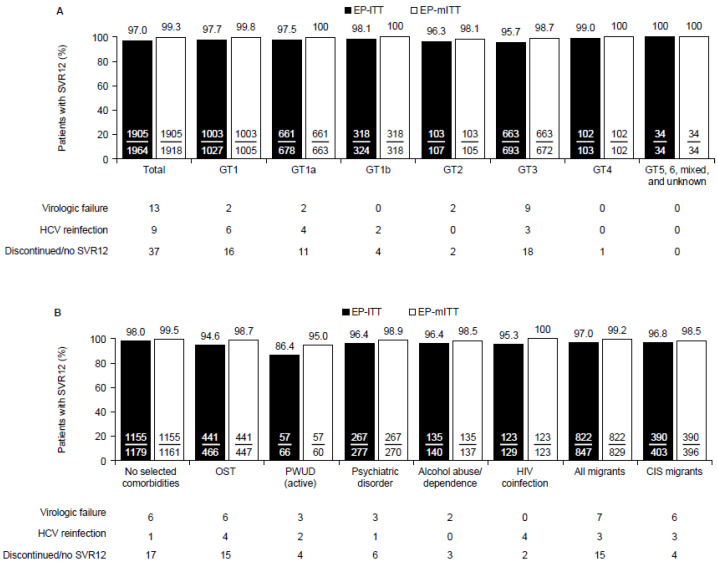
Using data from the German Hepatitis C-Registry (Deutsche Hepatitis C-Register, DHC-R), we report the real-world safety and effectiveness of glecaprevir/pibrentasvir (GLE/PIB) treatment and its impact on patient-reported outcomes (PROs) in underserved populations who are not typically included in clinical trials, yet who will be crucial for achieving hepatitis C virus (HCV) elimination. The DHC-R is an ongoing, non-interventional, multicenter, prospective, observational cohort study on patients treated for chronic HCV infection in Germany. The data cutoff was 17 January 2021. The primary effectiveness endpoint was sustained virologic response at post-treatment Week 12 (SVR12). Safety outcomes were assessed in all patients receiving GLE/PIB. PROs were assessed using the SF-36 survey. Of 2354 patients, 1964 had valid SVR12 data (intention-to-treat analysis). Of these, 1905 (97.0%) achieved SVR12 with rates similar across the comorbidities analyzed, except for people who actively use drugs (PWUD (active)) (86.4%). Excluding those who discontinued treatment and did not achieve SVR12, or were reinfected with HCV, the rate was 99.3%, with similar results regardless of comorbidity. PWUD (active) and those with psychiatric disorders had the most meaningful improvements in PROs. Adverse events (AEs) occurred in 631/2354 patients (26.8%), and serious AEs in 44 patients (1.9%). GLE/PIB was highly effective and well tolerated in this real-world study of patient groups key to HCV elimination.
Keywords: German Hepatitis C-Registry; direct-acting antiviral; glecaprevir/pibrentasvir; hepatitis C virus; real world evidence.
Conflict of interest statement
Markus Cornberg has served as a consultant/advisory board member/investigator/speaker for AbbVie, Gilead, GlaxoSmithKline, Janssen-Cilag, Merck/MSD, Novartis, Roche, Spring Bank Pharmaceuticals, and Swedish Orphan Biovitrum, and received research grants from Roche. Albrecht Stoehr has served as a speaker and advisory board member for AbbVie, Gilead, Janssen, Merck/MSD, Roche, and GSK/ViiV Healthcare. Uwe Naumann has served as a speaker/advisory board member for AbbVie, Gilead, Merck/MSD, Mundipharma, and GSK/ViiV Healthcare. Gerlinde Teuber has served as a speaker for AbbVie and BMS, and is on an advisory board for Janssen, Gilead, and Merck/MSD. Hartwig Klinker has served as a speaker and advisory board member for AbbVie, BMS, Gilead, Janssen, Merck/MSD, Pfizer, Shionogi, and GSK/ViiV Healthcare, and received research funding from AbbVie, Arrowhead, BMS, Gilead, Hector Foundation, Janssen, and Merck/MSD. Thomas Lutz received research funding from AbbVie, Gilead, GSK/ViiV Healthcare, Merck/MSD, and Heidelberg Immunotherpeutics. Hjördis Möller has no conflicts to disclose. Dennis Hidde and Kristina Lohmann are employees of AbbVie and may hold AbbVie stock or options. Karl-Georg Simon has served as a speaker/advisory board member for AbbVie, Falk, Gilead, Janssen, Merck/MSD, and Norgine.
Figures



References
-
- World Health Organization Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections. 2021. [(accessed on 3 May 2022)]. Available online: https://www.who.int/publications/i/item/9789240027077.
-
- Polaris Observatory German HCV Infections. [(accessed on 11 May 2021)]. Available online: https://cdafound.org/dashboard/polaris/dashboard.html.
-
- World Health Organization Global Health Sector Strategy on Viral Hepatitis 2016–2021. [(accessed on 3 May 2022)]. Available online: https://apps.who.int/iris/handle/10665/246177.
-
- World Health Organization Guidelines for the Care and Treatment of Persons Diagnosed with Chronic Hepatitis C Virus Infection. [(accessed on 3 May 2022)]. Available online: https://www.who.int/publications/i/item/9789241550345. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
